Professional Documents
Culture Documents
Cost - Effectiveness of Screening For Active Cases of Tuberculosis in Flanders, Belgium
Uploaded by
Renold CristianOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Cost - Effectiveness of Screening For Active Cases of Tuberculosis in Flanders, Belgium
Uploaded by
Renold CristianCopyright:
Available Formats
Research
Costeffectiveness of screening for active cases of tuberculosis in
Flanders, Belgium
G Suzanne A Smit,a Ludwig Apers,b Wouter Arrazola de Onate,c Philippe Beutels,d Pierre Dorny,b An-Marie Forier,e
Kristien Janssens,c Jean Macq,f Ruud Mak,e Sandrina Schol,c Dirk Wildemeersch,e Niko Speybroeckf &
Brecht Devleesschauwerg
Objective To assess the costeffectiveness of the tuberculosis screening activities currently funded by the Flemish government in Flanders,
Belgium.
Methods After estimating the expenses for 20132014 of each of nine screening components which include high-risk groups, contacts
and people who are seeking tuberculosis consultation at a centre for respiratory health care and the associated costs per active case of
tuberculosis identified between 2007 and 2014, we compared the costeffectiveness of each component. The applied perspective was
that of the Flemish government.
Findings The three most cost-effective activities appeared to be the follow-up of asylum seekers who were found to have abnormal X-rays
in initial screening at the Immigration Office, systematic screening in prisons and contact investigation. The mean costs of these activities
were 5564 (95% uncertainty interval, UI: 37918160), 11 603 (95% UI: 901014 909) and 13 941 (95% UI: 10 72318 201) euros () per
detected active case, respectively. The periodic or supplementary initial screening of asylum seekers and the screening of new immigrants
from high-incidence countries which had corresponding costs of 51 813 (95% UI: 34 85576 847), 126 236 (95% UI: 41 984347 822)
and 418 359 (95% UI: 74 9751 686 588) appeared much less cost-effective. Between 2007 and 2014, no active tuberculosis cases were
detected during screening in the juvenile detention centres.
Conclusion In Flanders, tuberculosis screening in juvenile detention centres and among new immigrants and the periodic or supplementary
initial screening of asylum seekers appear to be relatively expensive ways of detecting people with active tuberculosis.
Introduction all be contributing to an expansion in the burden posed by
tuberculosis.69
In 2014, the global incidence of tuberculosis was 133
If WHOs tuberculosis goal for 2035 is to be achieved,
cases per 100 000 population.1 The World Health Organization
global funding and commitment for tuberculosis care, control
(WHO) wishes to reduce the global incidence of tuberculosis
and prevention need to be increased10 and the cost-effective
below 10 cases per 100 000 population by 2035.2 Although the
use of the resources that are or become available has to
incidence in many high-income countries is already below
be optimized.11
this target level, tuberculosis remains a public health chal-
WHOs framework towards tuberculosis elimination in
lenge.3 In most low-incidence countries there are low rates of
low-incidence countries, provides further goals and a custom-
tuberculosis transmission among the native population, a de-
ized strategy for countries such as Belgium.6,12,13 According
veloping predominance of cases among the elderly and other
to this framework, interventions and target groups must be
vulnerable and hard-to-reach risk groups and individuals
prioritized based on an assessment of the epidemiology of
who carry latent tuberculosis infection for years before they
tuberculosis and health-care context in each setting that is
become symptomatic.4,5
guided by data analysis and operational research.6 We therefore
Low burdens of tuberculosis often lead to diminishing
evaluated the costeffectiveness of the tuberculosis screening
public awareness, inadequate political commitment, limited
activities, in northern Belgium, that are currently organized
clinical and diagnostic expertise and the underfunding of
and funded by the Flemish government. The reporting of this
tuberculosis research.4,6 At the same time, economic crises,
study conforms to the Consolidated Health Economic Evalu-
growing inequity, increases in the incidence of diseases
ation Reporting Standards (available from the corresponding
that are risk factors for tuberculosis and the dissemination
author).14
of drug-resistant forms of Mycobacterium tuberculosis may
a
Department of Virology, Parasitology and Immunology, Ghent University, Ghent, Belgium.
b
Institute of Tropical Medicine, Antwerp, Belgium.
c
Flemish Association for Respiratory Health and Tuberculosis Control, Brussels, Belgium.
d
Centre for Health Economics Research & Modelling Infectious Diseases, University of Antwerp, Antwerp, Belgium.
e
Agency for Care and Health, Government of Flanders, Brussels, Belgium.
f
Institute of Health and Society, Universit catholique de Louvain, Brussels, Belgium.
g
Scientific Institute of Public Health (WIV-ISP), Department of Public Health and Surveillance, Rue Juliette Wytsmanstraat 14, 1050 Brussels, Belgium.
Correspondence to Brecht Devleesschauwer (email: brecht.devleesschauwer@wiv-isp.be).
(Submitted: 11 January 2016 Revised version received: 30 August 2016 Accepted: 28 September 2016 Published online: 3 November 2016 )
Bull World Health Organ 2017;95:2735 | doi: http://dx.doi.org/10.2471/BLT.16.169383 27
Research
Costeffectiveness of tuberculosis screening in Belgium G Suzanne A Smit et al.
ously. Supplementary initial screening income lost and travel expenses during
Methods covers asylum seekers who are not eli- their illness.
Study setting gible for an X-ray e.g. children younger
than five years, the physically disabled
Estimated numbers
Flanders is the Dutch-speaking northern
part of Belgium and has about 6.4 million and pregnant women and those who are We assessed the number of people
inhabitants.15 The Flemish governments not screened at the Immigration Office screened and the number of active
Agency for Care and Health is respon- for other reasons. tuberculosis cases identified under the
sible for the general coordination of the In prisons that have their own X-ray current tuberculosis policy. To increase
tuberculosis policy in Flanders. It also facilities, the Justice Federal Public Ser- the reliability of our estimates, we
coordinates and partially carries out vice conducts the systematic screening included all cases detected in the pe-
and has the final responsibility for the of prisoners. In other prisons, the as- riod 20072014. However, for contact
investigation of contacts of individuals sociation conducts the screening, using investigation and follow-up of asylum
with infectious tuberculosis. Because a mobile X-ray unit. However, almost seekers, only data from 2013 and 2014
of resource constraints, a management all X-rays of prisoners in Flanders are were available.
contract was established between the read by the associations pulmonologists.
Compared with migrants in deten- tion
Costs
Flemish government and the Flemish
Association for Respiratory Health and centres or prisoners, other new We investigated the screening-related
Tuberculosis Control. The association immigrants are relatively hard to reach expenditure of the Agency for Care and
has its headquarters in Brussels and eight because they are very diverse in terms Health and the Flemish Association for
regional centres for respiratory health of the languages they speak and rapidly Respiratory Health and Tuberculosis
care in Flanders. On behalf of the Flem- disperse across Flanders. The associa- Control for the years 2013 and 2014.
ish government, the association carries tion develops leaflets for documented We used expert opinion to allocate
out active detection through contact immigrants, inviting them for screening. fixed costs e.g. overheads, rents, of-
investigation, systematic screening of The main goal of tuberculosis fice supplies, staff, and organizational
five high-risk groups and the screening screening in Flanders is the detection of development for each component
of other individuals hereafter simply active infectious pulmonary tuberculo- of the screening policy. Allocation
called others who, though they do not sis for which a chest X-ray represents weights were based on the percentage
belong to any specific risk groups, have the method of choice. However, for of time each employee working on the
presented for a consultation at a centre contact investigation and when inves- tuberculosis programme spent on each
for respiratory health care. tigating people who are not eligible for component. These percentages were re-
The high-risk groups that are an X-ray, initial screening is based on ported by the employees and recorded,
screened systematically but voluntarily a tuberculin skin test. If eligible for an anonymously, on questionnaires.
by the association are: (i) all asylum seek- X-ray, any contact found skin-test posi-
tive is subsequently investigated using a
Costeffectiveness
ers assigned to Flanders; (ii) all undocu-
mented migrants i.e. individuals lacking chest X-ray. For further diagnosis and Costeffectiveness was evaluated over
legal status in Belgium held in detention treatment, suspected tuberculosis pa- a one-year time horizon. With a policy
centres in Flanders; (iii) other immi- tients are referred to the curative sector. of non-intervention as the comparator,
grants who intend to stay in Flanders for The algorithms for the screening the incremental costeffectiveness ratio
more than three months and come from and treatment options that are provided for each implemented component of the
high-incidence countries i.e. countries in Belgium from the perspective of screening policy was defined as the ratio
that have more than 50 active cases of the high-risk groups, contacts of a con- of the annual cost, in euros (), over the
tuberculosis per 100 000 population; firmed case and others are available from period 20132014, to the annual num-
(iv) prisoners in Flanders; and (v) the the corresponding author. ber of active tuberculosis cases detected
youth held in juvenile detention centres We only looked at the effectiveness in the period 20072014. Using such
in Flanders. There is no legal obliga- of investments in tuberculosis control ratios, we compared the costeffective-
tion for screening people are invited made by the Flemish government and ness of each component. As we used
and strongly motivated but can refuse therefore only conducted our study from mean annual costs and outcomes, no
to participate. The associations screen- the perspective of the Agency for Care discounting was necessary.
ing of asylum seekers consists of three and Health and the Flemish Association
for Respiratory Health and Tuberculosis
Statistical analyses
components: (i) the follow-up of asylum
seekers found to have an abnormal chest Control. We ignored the costs of the Statistical uncertainty about the number
X-ray on initial screening by the Federal coordination and implementation of of detected tuberculosis cases and the
Agency for Asylum at the Immigration screening by the Federal Agency for costs was investigated using Dirichlet
Office16 hereafter called the follow-up of Asylum and the Justice Federal Public distributions and 10 000 Monte Carlo
asylum seekers; (ii) supplementary initial Service, the costs of diagnosis and simulations.17 We report the resulting
screening i.e. the screening of asylum treatment in the curative sector, the means and 95% uncertainty intervals
seekers who have not been investigated costs of tuberculosis screening within (UI). Data were collated into Excel 2010
by X-ray; and (iii) periodic screening, six programmes of occupational health care (Microsoft, Redmond, United States of
and 12 months after arrival, of those not and within hospitals and any indirect America) databases and analysed in R
known to have active tuberculosis previ- costs for tuberculosis patients e.g. version 3.2.0.18
28 Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383
Research
G Suzanne A Smit et al. Costeffectiveness of tuberculosis screening in Belgium
Table 1. Number of people screened and found positive for active tuberculosis and the associated costs, Flanders, Belgium, 2014
Screening component No. of people Estimated cost, in (95% UI)
Screened Identified as
active cases
Systematic screening of risk groups 12 832 28 471 283 (452 472490 462)
Asylum seekers 2 173 11 216 179 (200 572232 554)
Follow-up after initial screening at Immigration Office 164a 10 56 114 (52 61359 941)
Supplementary initial screening 195 0 36 980 (30 57943 926)
Periodic screening 1 814 1 123 085 (111 032135 824)
Undocumented migrants in detention centres 2 559 2 97 878 (85 806110 346)
Other immigrants from high-incidence countries 37 0 39 555 (32 18048 006)
Prisoners 7 901 15 113 325 (102 238125 148)
Youth in juvenile detention centres 162 0 4 346 (2 2597 613)
Contact investigation 3 872 34 395 224 (383 758407 242)
Screening others 835 3 80 207 (68 50692 833)
Total 17539 65 946714 (928711964892)
: Euro; UI: uncertainty interval.
a
In 2014, chest X-rays of 17 485 asylum seekers were taken at the Immigration Office by the Belgian Federal Agency for Asylum. The X-rays of 439 asylum seekers of
whom 164 were assigned to Flanders were considered abnormal.
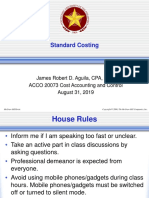
Results Fig. 1. Mean annual number of cases identified via each of nine components of the
Most (336; 82%) of the 410 people with screening for active cases of tuberculosis, Flanders, Belgium, 20072014
active tuberculosis reported in Flanders
in 2014 were detected passively, when
they sought health care. The other 74 Contact
people with active tuberculosis were investigation
detected during the screening of risk Asylum seekers
groups (28), contact investigation (34), follow-up
the screening of others (3) or by un- Prisoners
known means (9).12 Among the reported
Screening component
Undocumented
cases, 29 had been born in eastern Eu- migrants
rope and 208 outside Europe.
Table 1 summarizes the numbers Others
of people screened in 2014 via each Asylum seekers
component of the screening policy, periodic screening
the corresponding numbers of active Asylum seekers
tuberculosis cases detected and the supplementary initial screening
Other
related costs. Fig. 1 shows the mean
immigrants
annual numbers of active tuberculosis Juvenile detention
cases identified, via each component centres
of the screening policy, between 2007
0 10 20 30 40 50
and 2014. Over this period, in terms
Mean annual number of active cases detected
of the mean annual number of active
cases detected, contact investigation
Notes: Others include individuals who do not belong to any specific risk groups but presented for
appeared to be the most successful consultation at a centre for respiratory health care. The boxplots reflect the statistical uncertainty in the
component (mean: 28; 95% UI: 2136), mean annual number of detected cases. In each boxplot, the vertical line represents the median of all
followed by the follow-up of asylum simulated values, the box indicates the first and third quartiles, the whiskers extend to 1.5 times the
seekers (mean: 11; 95% UI: 816) and interquartile range, and the points represent simulated values outside that interval.
the screening of prisoners (mean: 10;
95% UI: 813). Over the same period, cases were identified during screening in 901014 909) and contact investigation
the supplementary initial screening of juvenile detention centres. (13 941; 95% UI: 10 72318 201). The
asylum seekers and the screening of The screening components found costs per case detected for the screening
other immigrants from high-incidence to have the lowest mean costs, per ac- of others and the systematic screening
countries only revealed a mean of 0.38 tive case detected (Fig. 2), were the of undocumented migrants in deten-
(95% UI: 0.100.83) and 0.18 (95% UI: follow-up of asylum seekers (5564; tion centres were relatively high, at
0.020.51) of an active case per year, 95% UI: 37918160), systematic screen- 25 337 (95% UI: 15 84340 343) and
respectively, while no active tuberculosis ing of prisoners (11 603; 95% UI: 28 474 (95% UI: 18 73442 439), re-
Bull World Health Organ 2017;95:2735 | doi: http://dx.doi.org/10.2471/BLT.16.169383 29
Research
Costeffectiveness of tuberculosis screening in Belgium G Suzanne A Smit et al.
tuberculosis control in the Nether-
Fig. 2. Costeffectiveness of each of nine components of the screening for active cases
lands includes an assessment of the
of tuberculosis, Flanders, Belgium, 20072014
costeffectiveness of each of the control
programmes components.22,23 Other
related investigations have tended to
Juvenile detention focus on the costeffectiveness of one
centres
specific screening component and/or
Other
immigrants the detection methods used.2427 One
Asylum seekers review indicated that screening of mi-
supplementary initial screening grants as they entered a low-incidence
Asylum seekers country was not very cost-effective and
Screening component
periodic screening had little impact on overall tuberculosis
Undocumented trends.25 In the Netherlands, the use of
migrants X-rays to screen immigrants on entry
Others has been shown to be cost-effective only
Contact for immigrants from areas where tuber-
investigation culosis incidence exceeds 300 cases per
100 000 population.23,28 As such screen-
Prisoners
ing appears to have little impact on the
Asylum seekers general epidemiology of tuberculosis in
follow-up the Netherlands, the detection of latent
0 10 000 100 000 1 000 000 10 000 000 100 000 000 tuberculosis infection in immigrant risk
ICER (cost in per active case detected) groups and the provision of accessible
preventive treatment may represent
: Euro; ICER: incremental costeffectiveness ratio. better uses of the resources available.29
Notes: Others include individuals who do not belong to any specific risk groups but presented for In the United Kingdom of Great Britain
consultation at a centre for respiratory health care. The boxplots reflect the statistical uncertainty in both and Northern Ireland, the post-entry
the mean annual cost and the mean annual number of detected cases. In each boxplot, the vertical
line represents the median of all simulated values, the box indicates the first and third quartiles, the
screening of immigrants for latent in-
whiskers extend to 1.5 times the interquartile range, and the points represent simulated values outside fection appeared to be cost-effective
that interval. No costeffectiveness ratio could be shown for the detection of cases during screening in when the immigrants targeted came
juvenile detention centres because between 2007 and 2014 no active cases were detected during such from countries with high incidence of
screening. tuberculosis.26 Little published informa-
tion exists on the costeffectiveness of
spectively. The corresponding costs for Our estimates of the costeffectiveness screening individuals who are very hard
the periodic screening (51 813; 95% of various other combinations of the to reach e.g. homeless people30,31 or
UI: 34 85576 847) and supplemen- screening components are available on the screening of prisoners.
tary initial screening of asylum seekers from the corresponding author. In Belgium, activities to detect, pre-
(126 236; 95% UI: 41 984347 822) vent and/or treat tuberculosis are carried
and the screening of other new immi- out by many different institutions, with
grants from high-incidence countries
Discussion many complex interactions. This study
(418 359; 95% UI: 74 9751 686 588) For the control of tuberculosis, WHO was conducted from the perspective of
were even higher. stresses the importance of priori- the Flemish Agency for Care and Health
In Fig. 3, we plotted costs on the tizing key interventions and target and the Flemish Association for Respira-
vertical axis and the number of identi- groups based on epidemiological and tory Health and Tuberculosis Control
fied active tuberculosis cases on the health-care system assessments and i.e. the institutions that, together, are
horizontal axis. The origin represents an evaluation of the benefits, risks and responsible for all of the tuberculosis
doing nothing i.e. no active screen- costs of each potentially useful interven- screening activities funded by the Flem-
ing. The line connects the origin with tion in each setting.6,19 Poorly targeted ish government. As it was not conducted
the policy component with the lowest systematic screening can be very ex- from a broad societal perspective, we
cost per case detected; as it runs to the pensive and ineffective20 and has little will have underestimated the total cost
right, each new data point represents epidemiological impact. 21 Screening of tuberculosis detection and prevention
the addition of another screening com- for active tuberculosis should therefore in Flanders.
ponent and the components are added be carefully targeted at groups with According to our estimates, in
in ascending order of the incremental the highest tuberculosis risk, and any Flanders, the follow-up of asylum seek-
costeffectiveness ratio. control programmes should incorporate ers represented the most cost-effective
In Flanders, a focus on the screen- measurements of effectiveness.19 component of the screening for active
ing of asylum seekers using a combina- Evaluations of the costeffective- tuberculosis. However, asylum seekers
tion of follow-up, supplementary initial ness of a complete tuberculosis screen- are only followed-up when they have
screening and periodic screening ing policy in terms of the costs per been both found to have an abnormal
would have cost about 15 729 (95% UI: active case detected are rare. An chest X-ray and assigned to Flanders.
11 40221 530) per active case detected. ongoing study to evaluate and optimize As people with abnormal chest X-rays
30 Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383
Research
G Suzanne A Smit et al. Costeffectiveness of tuberculosis screening in Belgium
sociation for Respiratory Health and
Fig. 3. Mean annual costs for and annual numbers of cases identified through
Tuberculosis Control, such immigrants
increasingly complex combinations of the components of screening for active
are at relatively low risk of tuberculo-
cases of tuberculosis, Flanders, Belgium, 20072014
sis. If this epidemiological assessment
changes, additional and more efficient
communication channels may become
1 000 000 necessary.37
+ Other immigrants Finally, since no active tuberculo-
+ Asylum seekerssupplementary initial screening sis cases were detected in the juvenile
+ Asylum seekersperiodic screening detention centres between 2007 and
2014, we were not able to calculate the
750 000 incremental costeffectiveness ratio
+ Undocumented migrants for this component. Although the cost
of taking a mobile X-ray unit to each
+ Others
detention centre once a year is not
Mean annual cost
+ Contact investigation particularly high compared with the
costs of the other policy components we
500 000 considered the fact that no cases were
detected in the detention centres over a
period of seven years makes the value of
this component questionable.
Disinvestment in one or more poli-
250 000 cy components should be supported by
a recent assessment of the epidemiology
+ Prisoners of tuberculosis in the setting involved.
Tuberculosis incidence may be affected
by changes in the influx of asylum seek-
+ Asylum seekersfollow-up
ers and immigrants. The number of first-
time asylum seekers who applied for
0 20 40 60
international protection in the European
Annual number of active cases detected
Union during the third quarter of 2015
was almost twice the number who ap-
: Euro. plied in the second quarter of the same
Note: Others include individuals who do not belong to any specific risk groups but presented for
consultation at a centre for respiratory health care. year: 413 800 versus 213 200. In Belgium
this trend was even more marked, with
a corresponding rise from 5040 in the
are relatively likely to have pulmonary initial screening was found to be the second quarter of 2015 to 14 650 in
tuberculosis, it is not surprising that a least cost-effective, followed by periodic the third.38 However, tuberculosis is
relatively high number of active cases screening. The costs of these two compo- not often transmitted from migrants to
were detected within the small group of nents, per active case detected, were very the resident population39 and WHOs
asylum seekers who were followed up. high and only exceeded by the costs Regional Office for Europe continues
Contact investigation is an essential of screening other immigrants mainly to provide support in response to the
component of tuberculosis control and because these activities revealed very migrant and refugee crisis.40 Possible
elimination strategies in most low- few active cases. Indeed, such screening cuts in public health spending and social
incidence countries. 32,33 In Flanders, is complicated by its voluntary nature protection may also permit increases in
34 (0.9%) and 556 (14%) of the 3872 and the difficulties in reaching targeted tuberculosis incidence and mortality.9,41
contact investigations in 2014 resulted individuals. WHO has recommended that ef-
in the diagnosis of active tuberculosis The screening of other new immi- forts to control tuberculosis in most
and latent tuberculosis infection, respec- grants from high-incidence countries countries be strengthened because the
tively (GSA Smit, personal communica- was found to be a particularly expensive global incidence of the disease is only
tion, 2015). The International Union method of identifying active cases of declining slowly while the threat posed
Against Tuberculosis and Lung Disease tuberculosis. Although there have been by multidrug resistance is growing.6,8,13
has encouraged the prioritization of efforts to increase the number of such However, as global incidence declines,
tuberculosis prevention and control in immigrants screened in Flanders via the detection of active cases becomes
penitentiary settings.34 Our estimates of networking, collaboration with relevant increasingly rare and, in consequence,
the costeffectiveness of the screening of intermediary organizations and the use the costeffectiveness of tuberculosis
prisoners were probably too low as they of invitations and leaflets the annual detection and prevention declines.
ignored the costs of X-ray screening by number of such immigrants who pres- Our conclusions are based on the
the Justice Federal Public Service. ent for screening has been declining.35,36 costeffectiveness of the current imple-
Among the screening activities for It is therefore fortunate that, according mentation of each main component of
asylum seekers, the supplementary to data for 2013 from the Flemish As- the Flemish policy on tuberculosis
Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383 31
Research
Costeffectiveness of tuberculosis screening in Belgium G Suzanne A Smit et al.
screening. However, the costeffective- tions. In reality, contact investigation is and/or detection rates will increase
ness of each main component can be unlikely to be fully independent of other efficiency.
altered by changes in each aspect of that screening components. To make more In Belgium, we recommend con-
component. If, for example, the Belgian accurate estimates of costeffectiveness tinuing contact investigation, the sys-
government were to change its definition of contact investigation, we need infor- tematic screening of prisoners and
of a country with a high incidence of tu- mation on how the infective cases i.e. the follow-up of asylum seekers with
berculosis e.g. by doubling the thresh- the sources are identified, the type of abnormal chest X-rays. Due to their
old to more than 100 cases per 100 000 risk group they represent if any and relatively high costs, per active tuber-
the costeffectiveness of screening im- how many contacts become infected culosis case identified, we also recom-
migrants from high-incidence countries per source. mend the re-evaluation of screening in
is likely to change markedly. Although health-care contexts juvenile detention centres, the screening
It may be beneficial to investigate and systems in many countries are of new immigrants and the periodic
the costeffectiveness of screening for not directly comparable, the methods and supplementary initial screening of
latent tuberculosis infection and the used in this study could be applied in asylum seekers.
effectiveness and costeffectiveness most low-incidence countries where
of the initial screening of all asylum the epidemiology and challenges are Acknowledgements
seekers regardless of their country generally similar to those in Flanders. GSAS and PD have dual appointments
of origin by the Federal Agency for Compared with passive detection, with, respectively, the Institute of Health
Asylum. In the control of tuberculosis, current programmes of active screen- and Society, Universit catholique de
some countries of origin of immigrants ing in low-incidence countries only Louvain, Brussels, Belgium and the
appear to be particularly challenging detect relatively small numbers of ac- Department of Virology, Parasitology
e.g. the Syrian Arab Republic has a tive tuberculosis cases and often at a and Immunology, Ghent University,
low reported incidence of tuberculosis high cost. The small numbers of active Ghent, Belgium.
but mass migration and war may have cases detected by active screening may
substantially increased incidence since reflect low numbers of active tubercu- Funding: This study was commissioned
the last nationwide survey.16 losis cases in the study population and/ and financially supported by the Flemish
Our study was limited by the con- or inefficient screening procedures. Agency for Care and Health.
sideration of contact investigation as an Implementation of different procedures
independent component in our calcula- that are cheaper and increase coverage Competing interests: None declared.
(13941 %95 -10723
.
)18201 .
- 2013 2014
51813 ( 95%
( 126236 )7684734855
418359
)1686588)347822-41984
74975
%95
%95
( 2007 2014
.
.
. 2007 2014
.
5564 (
.
. )8160
%95
-3791
11603(
)149090-9010 %95
20132014 9
9
32 Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383
Research
G Suzanne A Smit et al. Costeffectiveness of tuberculosis screening in Belgium
2007 2014
Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383 33
Research
Costeffectiveness of tuberculosis screening in Belgium G Suzanne A Smit et al.
X 347 822) 418 359 (95% UI: 74 9751 686 588)
5564 2007 2014
95% UI 37918160 11 603 (95% UI:
901014 909) 13 941 (95% UI: 10 72318 201)
51 813 (95%
UI: 34 85576 847)126 236 (95% UI: 41 984
Rsum
Rentabilit du dpistage des cas de tuberculose active en Flandre, en Belgique
Objectif valuer la rentabilit des activits de dpistage de la dincertitude de 95%, II: 37918160), 11 603 (II 95%: 901014 909)
tuberculose actuellement finances par le gouvernement flamand en et 13 941 (II 95%: 10 72318 201) euros () par cas actif dtect. Le
Flandre, en Belgique. dpistage initial priodique ou complmentaire des demandeurs
Mthodes Aprs avoir estim les dpenses pour 20132014 au titre de dasile et le dpistage des nouveaux immigrants originaires de pays
chacun des neuf composants du dpistage notamment les groupes forte incidence dont le cot tait respectivement de 51 813 (II 95%:
haut risque, les contacts et les personnes venant en consultation pour la 34 85576 847),126 236 (II95%:41 984347 822) et 418 359 (II 95%:
tuberculose dans un centre de traitement des problmes respiratoires 74 9751 686 588) se sont rvls beaucoup moins rentables. Entre
ainsi que les cots associs par cas de tuberculose active identifi entre 2007 et 2014, aucun cas de tuberculose active na t dtect lors du
2007 et 2014, nous avons compar la rentabilit de chaque composant. dpistage dans les centres de dtention pour mineurs.
La perspective applique tait celle du gouvernement flamand. Conclusion En Flandre, le dpistage de la tuberculose dans les centres
Rsultats Il est apparu que les trois activits les plus rentables taient de dtention pour mineurs et chez les nouveaux immigrants ainsi que
le suivi des demandeurs dasile dont les radiographies ralises lors le dpistage initial, priodique ou complmentaire, des demandeurs
du dpistage initial lOffice des trangers taient anormales, le dasile, est un moyen relativement coteux de dtecter les cas de
dpistage systmatique dans les prisons et la recherche des contacts. tuberculose active.
Le cot moyen de ces activits tait respectivement de 5564 (intervalle
11 603 (95%- : 901014 909) 13 941 (95%-
, : 10 72318 201)
, .
.
2013 2014
, ,
, , 51 813 (95%- :
34 85576 847), 126 236 (95%- : 41 984347 822)
, 418 359 (95%- : 74 9751 686 588),
, . 2007
2007 2014 , 2014
.
.
.
,
,
. .
5564 (95%- , : 37918160),
Resumen
Rentabilidad de los exmenes de deteccin de casos activos de tuberculosis en Flandes, Blgica
Objetivo Evaluar la rentabilidad de las actividades de deteccin de Mtodos Tras calcular los gastos de 20132014 de cada uno de los
tuberculosis actualmente financiadas por el gobierno flamenco en nueve componentes de los exmenes de deteccin (que incluyen
Flandes, Blgica. grupos de alto riesgo, contactos y personas que buscan consulta para la
34 Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383
Research
G Suzanne A Smit et al. Costeffectiveness of tuberculosis screening in Belgium
tuberculosis en un centro de atencin respiratoria) y los costes asociados inicial peridicos o complementarios de los buscadores de asilo y los
por caso activo de tuberculosis identificados entre 2007 y 2014, se exmenes de deteccin de los nuevos inmigrantes de pases con una
compar la rentabilidad de cada componente. Se aplic la perspectiva alta incidencia (con costes correspondientes de 51 813 (II del 95%:
del gobierno flamenco. 34 85576 847), 126 236 (II del 95%: 41 984347 822) y 418 359 (II del
Resultados Parece que las tres actividades ms rentables fueron el 95%: 74 9751 686 588) euros) parecieron ser mucho menos rentables.
seguimiento de los buscadores de asilo con unas radiografas poco Entre 2007 y 2014 no se detectaron casos de tuberculosis activa durante
habituales en el examen de deteccin inicial en la Oficina de Inmigracin, los exmenes de deteccin en centros penitenciarios juveniles.
los exmenes de deteccin sistemticos en prisiones y la investigacin Conclusin En Flandes, los exmenes de deteccin de tuberculosis
de contactos. Los costes medios de estas actividades fueron de 5 564 en centros penitenciarios juveniles y aquellos realizados entre nuevos
(intervalo de incertidumbre, II, del 95%: 3 7918 160), 11 603 (II del inmigrantes, as como los exmenes de deteccin inicial peridicos
95%: 9 01014 909) y 13 941 (II del 95%: 10 72318 201) euros () por o complementarios de los buscadores de asilo, parecen ser formas
caso activo detectado respectivamente. Los exmenes de deteccin relativamente caras de detectar a personas con tuberculosis activa.
References
1. Global Tuberculosis Report 2015. Geneva: World Health 16. Arrazola de Onate W, Weber L, Janssens K, Wanlin M, Forier A, Schol
Organization; 2015. Available from: http://apps.who.int/iris/ S, et al. Tuberculosis screening yield of asylum seekers in Europe
bitstream/10665/191102/1/9789241565059_eng.pdf [cited 2016 Oct 20]. correspondence. Eur Respir J. 2016;48(4):12. doi: http://dx.doi.
2. Global strategy and targets for tuberculosis prevention, care and control org/10.1183/13993003.00991-2016 PMID: 27365500
after 2015. Sixty-seventh World Health Assembly Resolution A67/11. 17. Bilcke J, Beutels P,Brisson M, Jit M. Accounting for methodological,
Geneva: World Health Organization; 2014. structural, and parameter uncertainty in decision-analytic models: a
3. Lnnroth K, Jaramillo E, Williams BG, Dye C, Raviglione M. Drivers of practical guide. Med Decis Making. 2011 Jul-Aug;31(4):67592. doi: http://
tuberculosis epidemics: the role of risk factors and social determinants. dx.doi.org/10.1177/0272989X11409240 PMID: 21653805
Soc Sci Med. 2009 Jun;68(12):22406. doi: http://dx.doi.org/10.1016/j. 18. R: a language and environment for statistical computing. Vienna: R Core
socscimed.2009.03.041 PMID: 19394122 Team, R Foundation for Statistical Computing; 2015. Available from: http://
4. DAmbrosio L, Dara M, Tadolini M, Centis R, Sotgiu G, van der Werf MJ, et al.; www.R-project.org/ [cited 2016 Jan 6].
European national programme representatives. Tuberculosis elimination: 19. Systematic screening for active tuberculosis principles and
theory and practice in Europe. Eur Respir J. 2014 May;43(5):141020. doi: recommendations. Geneva: World Health Organization; 2013.
http://dx.doi.org/10.1183/09031936.00198813 PMID: 24389868 20. Vant Hoog AH, Onozaki I, Lnnroth K. Choosing algorithms for TB
5. Dara M, de Colombani P,Petrova-Benedict R, Centis R, Zellweger JP, screening: a modelling study to compare yield, predictive value and
Sandgren A, et al.; Wolfheze Transborder Migration Task Force. Minimum diagnostic burden. BMC Infect Dis. 2014;14(1):532. doi: http://dx.doi.
package for cross-border TB control and care in the WHO European region: org/10.1186/1471-2334-14-532 PMID: 25326816
a Wolfheze consensus statement. Eur Respir J. 2012 Nov;40(5):108190. doi: 21. Kranzer K, Afnan-Holmes H, Tomlin K, Golub JE, Shapiro AE, Schaap A, et
http://dx.doi.org/10.1183/09031936.00053012 PMID: 22653772 al. The benefits to communities and individuals of screening for active
6. Framework towards tuberculosis elimination in low-incidence countries. tuberculosis disease: a systematic review. Int J Tuberc Lung Dis. 2013
Geneva: World Health Organization; 2014. Apr;17(4):43246. doi: http://dx.doi.org/10.5588/ijtld.12.0743 PMID:
7. Creswell J, Raviglione M, Ottmani S, Migliori GB, Uplekar M, Blanc L, et al. 23485377
Tuberculosis and noncommunicable diseases: neglected links and missed 22. de Vries G, Baltussen R. The cost of tuberculosis and tuberculosis control.
opportunities. Eur Respir J. 2011 May;37(5):126982. doi: http://dx.doi. Infectieziekten Bull. 2013;24:13640. Dutch.
org/10.1183/09031936.00084310 PMID: 20947679 23. Report of the joint WHO and ECDC programme review of the national TB
8. Nathanson E, Nunn P, Uplekar M, Floyd K, Jaramillo E, Lnnroth K, et al. control programme in the Netherlands 2013. Copenhagen: World Health
MDR tuberculosis critical steps for prevention and control. N Engl J Med. Organization Regional Office for Europe; 2014. Available from: http://
2010 Sep 9;363(11):10508. doi: http://dx.doi.org/10.1056/NEJMra0908076 www.euro.who.int/ data/assets/pdf_file/0006/255354/Report-of-the-
PMID: 20825317 joint-WHO-and-ECDC-programme-review-of-the-national-TB-control-
9. Reeves A, Basu S, McKee M, Sandgren A, Stuckler D, Semenza JC. programme-in-the-Netherlands.pdf [cited 2016 Feb 8].
Tuberculosis control and economic recession: longitudinal study of data 24. Erkens CG, Dinmohamed AG, Kamphorst M, Toumanian S, van Nispen-
from 21 European countries, 19912012. Bull World Health Organ. 2015 Dobrescu R, Alink M, et al. Added value of interferon-gamma release assays
Jun 1;93(6):36979. doi: http://dx.doi.org/10.2471/BLT.14.142356 PMID: in screening for tuberculous infection in the Netherlands. Int J Tuberc Lung
26240458 Dis. 2014 Apr;18(4):41320. doi: http://dx.doi.org/10.5588/ijtld.13.0589
10. Floyd K, Pantoja A. Financial resources required for tuberculosis control PMID: 24670695
to achieve global targets set for 2015. Bull World Health Organ. 2008 25. Dasgupta K, Menzies D. Costeffectiveness of tuberculosis control strategies
Jul;86(7):56876. doi: http://dx.doi.org/10.2471/BLT.07.049767 PMID: among immigrants and refugees. Eur Respir J. 2005 Jun;25(6):110716. doi:
18670669 http://dx.doi.org/10.1183/09031936.05.00074004 PMID: 15929967
11. Verdier JE, de Vlas SJ, Baltussen R, Richardus JH. A systematic review of 26. Pareek M, Watson JP, Ormerod LP, Kon OM, Woltmann G, White PJ, et al.
economic evaluation studies of tuberculosis control in high-income Screening of immigrants in the UK for imported latent tuberculosis: a
countries. Int J Tuberc Lung Dis. 2011 Dec;15(12):158798. doi: http:// multicentre cohort study and costeffectiveness analysis. Lancet Infect
dx.doi.org/10.5588/ijtld.10.0332 PMID: 21740647 Dis. 2011 Jun;11(6):43544. doi: http://dx.doi.org/10.1016/S1473-
12. Tuberculosis register. Brussels: Flemish Association for Respiratory Health 3099(11)70069-X PMID: 21514236
and Tuberculosis Control; 2014. Dutch. 27. Zenner D, Southern J, van Hest R, DeVries G, Stagg HR, Antoine D, et al.
13. Global tuberculosis database [Internet]. Geneva: World Health Organization. Active case finding for tuberculosis among high-risk groups in low-
Available from: http://who.int/tb/country/data/download/en/ [cited 2015 incidence countries. Int J Tuberc Lung Dis. 2013 May;17(5):57382. doi:
Jul 7]. http://dx.doi.org/10.5588/ijtld.12.0920 PMID: 23575321
14. Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et 28. Van Rest JF, Erkens CGM, de Vries G. Evaluation of the tuberculosis
al.; CHEERS Task Force. Consolidated Health Economic Evaluation Reporting screening of immigrants in the Netherlands, 2005-2010. The Hague:
Standards (CHEERS) statement. Value Health. 2013 Mar-Apr;16(2):e15. doi: KNCV Tuberculosis Foundation; 2012. Available from: https://www.
http://dx.doi.org/10.1016/j.jval.2013.02.010 PMID: 23538200 kncvtbc.org/uploaded/2016/01/evaluatie_tuberculosescreening_
15. Population by place of residence, nationality, marital status, age and immigranten_2005-2010.pdf [cited 2016 Feb 8]. Dutch.
sex 1 January 2015. Brussels: Federal Public Service Economy; 2015. 29. Erkens C, Verhagen M. Discussion about TB screening of immigrants. Tegen
Available from: https://bestat.economie.fgov.be/bestat/crosstable. Tuberc. 2014;110(2):101. Dutch.
xhtml?datasource=65ee413b-3859-4c6f-a847-09b631766fa7 [cited 2016
Jan 6]. Dutch.
Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383 35
Research
Costeffectiveness of tuberculosis screening in Belgium G Suzanne A Smit et al.
30. Jit M, Stagg HR, Aldridge RW, White PJ, Abubakar I; Find and Treat 37. Tuberculosis register. Brussels: Flemish Association for Respiratory Health
Evaluation Team. Dedicated outreach service for hard to reach patients with and Tuberculosis Control; 2013. Available from: http://www.vrgt.be/
tuberculosis in London: observational study and economic evaluation. BMJ. uploads/documentenbank/28bf5af1188e3e5846bbce9db29bf728.pdf
2011;343 sep13 5:d53765376. doi: http://dx.doi.org/10.1136/bmj.d5376 [cited 2016 Jan 6]. Dutch.
PMID: 22067473 38. Asylum in the EU Member States. More than 410 000 first time asylum
31. Kimerling ME, Shakes CF, Carlisle R, Lok KH, Benjamin WH, Dunlap NE. Spot seekers registered in the third quarter of 2015. 1 out of 3 are from Syria.
sputum screening: evaluation of an intervention in two homeless shelters. Luxembourg: Eurostat; 2015. Available from: http://ec.europa.eu/eurostat/
Int J Tuberc Lung Dis. 1999 Jul;3(7):6139. PMID: 10423224 documents/2995521/7105334/3-10122015-ap-en.pdf/04886524-58f2-
32. Recommendations for investigating the contacts of persons with infectious 40e9-995d-d97520e62a0e [cited 2016 Jan 4].
tuberculosis in low- and middle-income countries. Geneva: World Health 39. Kamper-Jrgensen Z, Andersen AB, Kok-Jensen A, Kamper-Jrgensen
Organization; 2012. M, Bygbjerg IC, Andersen PH, et al. Migrant tuberculosis: the extent of
33. Erkens CGM, Kamphorst M, Abubakar I, Bothamley GH, Chemtob D, Haas transmission in a low burden country. BMC Infect Dis. 2012;12(1):60. doi:
W, et al. Tuberculosis contact investigation in low prevalence countries: a http://dx.doi.org/10.1186/1471-2334-12-60 PMID: 22423983
European consensus. Eur Respir J. 2010 Oct;36(4):92549. doi: http://dx.doi. 40. Migration and health: key issues [Internet]. Geneva: World Health
org/10.1183/09031936.00201609 PMID: 20889463 Organization; 2015. Available from: http://www.euro.who.int/en/health-
34. Dara M, Chadha SS, Vinkeles Melchers NV, van den Hombergh J, Gurbanova topics/health-determinants/migration-and-health/news/news/2015/09/
E, Al-Darraji H, et al.; International Union Against Tuberculosis and Lung population-movement-is-a-challenge-for-refugees-and-migrants-as-well-
Disease. Time to act to prevent and control tuberculosis among inmates. Int as-for-the-receiving-population/migration-and-health-key-issues [cited
J Tuberc Lung Dis. 2013 Jan;17(1):45. PMID: 23231999 2016 Jan 4].
35. Annual report on tuberculosis detection and control in the Flemish region. 41. Reeves A, Basu S, McKee M, Stuckler D, Sandgren A, Semenza J. Social
Brussels: Flemish Association for Respiratory Health and Tuberculosis protection and tuberculosis control in 21 European countries, 19952012:
Control; 2013. Dutch. a cross-national statistical modelling analysis. Lancet Infect Dis. 2014
36. Annual report on tuberculosis detection and control in the Flemish region. Nov;14(11):110512. doi: http://dx.doi.org/10.1016/S1473-3099(14)70927-
Brussels: Flemish Association for Respiratory Health and Tuberculosis 2 PMID: 25303845
Control; 2014. Dutch.
36 Bull World Health Organ 2017;95:2735| doi: http://dx.doi.org/10.2471/BLT.16.169383
You might also like
- The World of The GerDocument302 pagesThe World of The GerMystic Master0% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- The Rights of Man and The Tyranny of LawDocument12 pagesThe Rights of Man and The Tyranny of LawSancrucensisNo ratings yet
- Acute TonsillitisDocument22 pagesAcute Tonsillitisg0ldz21100% (10)
- 158 Carino vs. CADocument2 pages158 Carino vs. CAFrancesca Isabel Montenegro67% (3)
- UEFA Stadium Design Guidelines PDFDocument160 pagesUEFA Stadium Design Guidelines PDFAbdullah Hasan100% (1)
- Bay Marshalling BoxesDocument4 pagesBay Marshalling BoxesSimbu ArasanNo ratings yet
- Ayurveda Secrets of Healing Maya Tiwari.07172 2seasonal CleansingDocument5 pagesAyurveda Secrets of Healing Maya Tiwari.07172 2seasonal CleansingkidiyoorNo ratings yet
- DOTSDocument3 pagesDOTSTammy Utami DewiNo ratings yet
- Diagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsDocument16 pagesDiagnosis & Treatment of Tuberculosis in HIV Co-Infected PatientsdevisilalahiNo ratings yet
- Early Detection of Tuberculosis Through Community-Based Active Case Finding in CambodiaDocument11 pagesEarly Detection of Tuberculosis Through Community-Based Active Case Finding in CambodiaPatriciann13No ratings yet
- Faq Tbhiv PolicyDocument4 pagesFaq Tbhiv PolicyviniganorNo ratings yet
- I. EPI Updates and TrendsDocument3 pagesI. EPI Updates and TrendsChristine AlmoraNo ratings yet
- Child Health and TBDocument3 pagesChild Health and TBsoukumar8305No ratings yet
- CDC 8044 DS1Document8 pagesCDC 8044 DS1immanueldioNo ratings yet
- 13-10 Topic 7. Complicated PneumoniaDocument35 pages13-10 Topic 7. Complicated PneumoniaReza Ervanda ZilmiNo ratings yet
- TB in ChildrenDocument9 pagesTB in Childrenparamita nindyaNo ratings yet
- Nihpp rs3758745v1Document20 pagesNihpp rs3758745v1Yulia Niswatul FauziyahNo ratings yet
- Asmer Khalid OmerDocument8 pagesAsmer Khalid OmerEsmer XalîdNo ratings yet
- TB DR MohabbatDocument27 pagesTB DR Mohabbatdr_hammadNo ratings yet
- Shingadia 2003Document9 pagesShingadia 2003syifa fileNo ratings yet
- Chapter 1: Introduction and Diagnosis of Tuberculosis in ChildrenDocument7 pagesChapter 1: Introduction and Diagnosis of Tuberculosis in ChildrenEster SibaraniNo ratings yet
- CAP Guidelines SA 2020Document22 pagesCAP Guidelines SA 2020kudzaimuregidubeNo ratings yet
- Tuberculosis Surveillance: Data For Decision-Making: EditorialcommentaryDocument3 pagesTuberculosis Surveillance: Data For Decision-Making: EditorialcommentaryMuhammad Hafiidh MuizzNo ratings yet
- Tuberculosis in Pregnancy: Review ArticleDocument6 pagesTuberculosis in Pregnancy: Review ArticleMustika OktariniNo ratings yet
- Free Tuberculosis Research PaperDocument6 pagesFree Tuberculosis Research Papermkrferqhf100% (1)
- 2015 Article 53Document7 pages2015 Article 53odyNo ratings yet
- International Journal of Infectious Diseases: Ben J. MaraisDocument4 pagesInternational Journal of Infectious Diseases: Ben J. MaraisMiftahurrahmah GmsNo ratings yet
- Novitasari - Is Premigration Health Screening For Tuberculosis WorthwileDocument12 pagesNovitasari - Is Premigration Health Screening For Tuberculosis Worthwileontet28No ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundEgi NabilaNo ratings yet
- Placement Report: Good Shepherd Hospital, SwazilandDocument22 pagesPlacement Report: Good Shepherd Hospital, SwazilandNaftal ShetunyengaNo ratings yet
- Research On Prevalence of TB FinalDocument9 pagesResearch On Prevalence of TB FinalBontuNo ratings yet
- Review 1Document23 pagesReview 1ms. chokyuNo ratings yet
- CHN - M3Document29 pagesCHN - M3Kristine KimNo ratings yet
- Tuberculosis and HIV Infection: The Global Setting: SupplementarticleDocument10 pagesTuberculosis and HIV Infection: The Global Setting: SupplementarticleCaster BondoNo ratings yet
- Jurnal RadiologiDocument9 pagesJurnal RadiologiAndrean HeryantoNo ratings yet
- 4-Mycology. 7.1.2024Document10 pages4-Mycology. 7.1.2024Ayob AlarabiNo ratings yet
- The Possible Causes of Misdiagnosed Pulmonary Tuberculosis Cases in The PhilippinesDocument2 pagesThe Possible Causes of Misdiagnosed Pulmonary Tuberculosis Cases in The PhilippinesAshNo ratings yet
- Management of Vaginal Discharge Syndrome: How Effective Is Our Strategy?Document4 pagesManagement of Vaginal Discharge Syndrome: How Effective Is Our Strategy?Epi PanjaitanNo ratings yet
- Recent Developments in The Diagnosis and Management of TuberculosisDocument8 pagesRecent Developments in The Diagnosis and Management of TuberculosisRhahahaNo ratings yet
- Usia TBDocument9 pagesUsia TBViviNo ratings yet
- The Epidemiology of Childhood Tuberculosis in The Netherlands: Still Room For PreventionDocument9 pagesThe Epidemiology of Childhood Tuberculosis in The Netherlands: Still Room For PreventionRivani KurniawanNo ratings yet
- Fuchs 2018Document14 pagesFuchs 2018Miguel Angel CayojaNo ratings yet
- Jurnal TBC Inter 1Document5 pagesJurnal TBC Inter 1sekti lindaNo ratings yet
- Clinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisDocument9 pagesClinical Manifestations of Human Brucellosis: A Systematic Review and Meta-AnalysisgustiNo ratings yet
- 420 068 Guideline PolioAFMDocument23 pages420 068 Guideline PolioAFMHusain TamimieNo ratings yet
- Kyuon Woo CI Medidas AdministrativasDocument6 pagesKyuon Woo CI Medidas AdministrativasVigilancia EpidemiologicaNo ratings yet
- TB CHildren Perez-Velez2017Document10 pagesTB CHildren Perez-Velez2017imil irsalNo ratings yet
- 2014 Clinical Toolkit 6 - Emergency Department Management of Paediatric SepsisDocument21 pages2014 Clinical Toolkit 6 - Emergency Department Management of Paediatric SepsisNisar ShaikNo ratings yet
- 1571 FullDocument11 pages1571 FullRai Pati FahleviNo ratings yet
- 1 s2.0 S2173511517301550 MainDocument6 pages1 s2.0 S2173511517301550 MainHermenegildo chitumbaNo ratings yet
- Literature Review of Pneumonia Under Five YearDocument6 pagesLiterature Review of Pneumonia Under Five Yeare9xy1xsv100% (1)
- Transient Hyperglycemia in Patients With Tuberculosis in Tanzania: Implications For Diabetes Screening AlgorithmsDocument10 pagesTransient Hyperglycemia in Patients With Tuberculosis in Tanzania: Implications For Diabetes Screening AlgorithmsNura RamadhanNo ratings yet
- Cancer Medicine - 2024 - Gorasso - The Incremental Healthcare Cost Associated With Cancer in Belgium A Registry Based DataDocument9 pagesCancer Medicine - 2024 - Gorasso - The Incremental Healthcare Cost Associated With Cancer in Belgium A Registry Based DataprimaNo ratings yet
- Ijerph 18 08373 v2Document14 pagesIjerph 18 08373 v2Huy Trần ThiệnNo ratings yet
- 2000 - WHO DOTS and Multidrug Resistant Tuberculosis Are Any Modifications RequiredDocument23 pages2000 - WHO DOTS and Multidrug Resistant Tuberculosis Are Any Modifications RequiredTammy Utami DewiNo ratings yet
- Early Detection of TBDocument32 pagesEarly Detection of TBAlfonso HasudunganNo ratings yet
- Quality of Nurs-WPS OfficeDocument2 pagesQuality of Nurs-WPS OfficeLjc JaslinNo ratings yet
- Thesis About Tuberculosis in The PhilippinesDocument6 pagesThesis About Tuberculosis in The PhilippinesPapersWritingServiceFortWayne100% (1)
- Tbhiv Infectioncontrol AddendumDocument43 pagesTbhiv Infectioncontrol AddendumBich Le Thi NgocNo ratings yet
- Further Efforts in The Achievement of Congenital Rubella Syndrome/rubella EliminationDocument5 pagesFurther Efforts in The Achievement of Congenital Rubella Syndrome/rubella Eliminationfpm5948No ratings yet
- JurnalDocument7 pagesJurnalBimaSuryaNo ratings yet
- Risk Factors For Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewDocument11 pagesRisk Factors For Community-Acquired Pneumonia in Adults in Europe: A Literature ReviewKorwin TitlaNo ratings yet
- MUSIMENTDocument4 pagesMUSIMENTMulongo LinoNo ratings yet
- FMF ProposalDocument2 pagesFMF ProposalFrance PalNo ratings yet
- Prisons and Health, 9 Infectious Diseases in PrisonDocument8 pagesPrisons and Health, 9 Infectious Diseases in PrisonBam ManNo ratings yet
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?From EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?No ratings yet
- 125) League of Cities of The Philippines vs. COMELEC (G.R. No. 176951, April 12, 2011) 2Document35 pages125) League of Cities of The Philippines vs. COMELEC (G.R. No. 176951, April 12, 2011) 2Carmel Grace KiwasNo ratings yet
- Flexible Evaluation Mechanism (FEM) Understanding Culture Society and PoliticsDocument1 pageFlexible Evaluation Mechanism (FEM) Understanding Culture Society and Politicsgenesisgamaliel montecinoNo ratings yet
- TC1 Response To A Live Employer Brief: Module Code: BSOM084Document16 pagesTC1 Response To A Live Employer Brief: Module Code: BSOM084syeda maryemNo ratings yet
- 08 03 Runge-Kutta 2nd Order MethodDocument11 pages08 03 Runge-Kutta 2nd Order MethodJohn Bofarull GuixNo ratings yet
- Simple Past News Biography Regular and Irregular VerbsDocument15 pagesSimple Past News Biography Regular and Irregular VerbsDaniela MontemayorNo ratings yet
- Graduate Alumni of Elvel School Class of 1991Document3 pagesGraduate Alumni of Elvel School Class of 1991Ramón SilvaNo ratings yet
- DPC Rough Draft by Priti Guide (1953)Document6 pagesDPC Rough Draft by Priti Guide (1953)Preeti GuideNo ratings yet
- CS302 - Lab Manual - Week No PDFDocument8 pagesCS302 - Lab Manual - Week No PDFattiqueNo ratings yet
- 8.31 - Standard CostingDocument109 pages8.31 - Standard CostingBhosx Kim100% (1)
- Indian Standard: General Technical Delivery Requirements FOR Steel and Steel ProductsDocument17 pagesIndian Standard: General Technical Delivery Requirements FOR Steel and Steel ProductsPermeshwara Nand Bhatt100% (1)
- LESSON 1 Overview of Toeic Speaking WritingDocument29 pagesLESSON 1 Overview of Toeic Speaking WritingPhạm Thị HuyềnNo ratings yet
- Product and Services: Karmic Nakshatras in Tamil AstrologyDocument4 pagesProduct and Services: Karmic Nakshatras in Tamil AstrologySushant ChhotrayNo ratings yet
- Opening Evolution by Bill WallDocument11 pagesOpening Evolution by Bill WallKartik ShroffNo ratings yet
- Karrnathi Undead P2Document2 pagesKarrnathi Undead P2Monjis MonjasNo ratings yet
- Mechanics of Materials Lab 1-Zip Tie Tensile TestingDocument7 pagesMechanics of Materials Lab 1-Zip Tie Tensile TestingcoolshavaNo ratings yet
- Sample Legal Advice Problems and AnswersDocument4 pagesSample Legal Advice Problems and AnswersJake Bryson DancelNo ratings yet
- Interjections Worksheet PDFDocument1 pageInterjections Worksheet PDFLeonard Patrick Faunillan Bayno100% (1)
- PPHNDocument32 pagesPPHNAnonymous NeRC5JYiSNo ratings yet
- Dina Iordanova - Women in Balkan Cinema, Surviving On The MarginsDocument17 pagesDina Iordanova - Women in Balkan Cinema, Surviving On The MarginsimparatulverdeNo ratings yet
- Azevedo Slum English 1926Document90 pagesAzevedo Slum English 1926Nealon Isaacs100% (1)
- SVFC BS Accountancy - 2nd Set Online Resources SY20-19 2nd Semester PDFDocument14 pagesSVFC BS Accountancy - 2nd Set Online Resources SY20-19 2nd Semester PDFLorraine TomasNo ratings yet
- ESpace EMS Product Description (V200R001C02SPC200 - 04)Document53 pagesESpace EMS Product Description (V200R001C02SPC200 - 04)Beatriz RomanNo ratings yet
- Cs6109 - Compiler Design: Lab AssignmentDocument8 pagesCs6109 - Compiler Design: Lab AssignmentvezhaventhanNo ratings yet