You might also like
- Latin Eugenics in Comparative PerspectiveDocument356 pagesLatin Eugenics in Comparative PerspectivemafeNo ratings yet
- ACLS Pretest Exam AnnotatedDocument21 pagesACLS Pretest Exam AnnotatedMOLLYNo ratings yet
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDocument6 pagesHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNo ratings yet
- Patellofemoral Pain SyndromeDocument21 pagesPatellofemoral Pain SyndromeAdvanced Physiotherapy100% (1)
- IsometricsDocument3 pagesIsometricsgtlaau100% (1)
- Behavioural ScienceDocument10 pagesBehavioural SciencecindyNo ratings yet
- 2012 Ankle Proprioception Is Not Targeted by Exercises On An Unstable SurfaceDocument10 pages2012 Ankle Proprioception Is Not Targeted by Exercises On An Unstable SurfaceMaría Pía Aravena CastilloNo ratings yet
- Logistics Management Plan FormatDocument10 pagesLogistics Management Plan FormatAnna BelleNo ratings yet
- Diagnostic Value of Five Clinical Tests in Patellofemoral Pain SyndromeDocument9 pagesDiagnostic Value of Five Clinical Tests in Patellofemoral Pain Syndromesridhar100% (1)
- Net Jets Pilot & Benefits PackageDocument4 pagesNet Jets Pilot & Benefits PackagedtoftenNo ratings yet
- Business Plan SampleDocument14 pagesBusiness Plan SampleErvin Evangelista100% (1)
- Effects of Posterior X Taping On Movement Quality and Knee Pain Intensity During Forward-Step-Down in Patients With Patellofemoral Pain SyndromeDocument7 pagesEffects of Posterior X Taping On Movement Quality and Knee Pain Intensity During Forward-Step-Down in Patients With Patellofemoral Pain Syndromesaeed seedNo ratings yet
- A Comparison of Hip Strength Between Sedentary Females With and Without PFPS PDFDocument7 pagesA Comparison of Hip Strength Between Sedentary Females With and Without PFPS PDFElaine CspNo ratings yet
- Effect of Static Knee Joint Flexion On Vastus Medialis Obliquus Fiber Angle in Patellofemoral Pain Syndrome - An Ultrasonographic StudyDocument9 pagesEffect of Static Knee Joint Flexion On Vastus Medialis Obliquus Fiber Angle in Patellofemoral Pain Syndrome - An Ultrasonographic Studycris weeNo ratings yet
- 2004 Patellar Taping Increases Vastus Medialis Oblique Activity in The Presence of Patellofemoral PainDocument10 pages2004 Patellar Taping Increases Vastus Medialis Oblique Activity in The Presence of Patellofemoral PainWei HungNo ratings yet
- Opciones de Atritis PT 2022Document17 pagesOpciones de Atritis PT 2022saraNo ratings yet
- Signorile2014 PDFDocument10 pagesSignorile2014 PDFErnestoNo ratings yet
- Ankle Muscle Activity Modulation During Single-Leg Stance Differs Between Children, Young Adults and SeniorsDocument9 pagesAnkle Muscle Activity Modulation During Single-Leg Stance Differs Between Children, Young Adults and SeniorsTadija TrajkovićNo ratings yet
- Manual Therapy: Theresa Helissa Nakagawa, Carlos Dias Maciel, F Abio Viadanna Serr AoDocument5 pagesManual Therapy: Theresa Helissa Nakagawa, Carlos Dias Maciel, F Abio Viadanna Serr AoHusna LathiifaNo ratings yet
- Jospt 2009 2885 PDFDocument8 pagesJospt 2009 2885 PDFItai IzhakNo ratings yet
- Rodilla 1Document7 pagesRodilla 1AdosotoNo ratings yet
- The Role of Muscle Strength & Activation Patterns in Patellofemoral PainDocument5 pagesThe Role of Muscle Strength & Activation Patterns in Patellofemoral Paincristian fabian perez romeroNo ratings yet
- 296Document9 pages296pokharelriwaj82No ratings yet
- The Effect of Closed Kinetic Chain Exercises And.14Document7 pagesThe Effect of Closed Kinetic Chain Exercises And.14fgomez235No ratings yet
- Dix HallPike TestDocument2 pagesDix HallPike TestnvalenzuelanNo ratings yet
- Does Experimental Low Back Pain Change PDocument8 pagesDoes Experimental Low Back Pain Change PJuancepaNo ratings yet
- 2011 Longstanding Adduction-Related Groin Pain in Athletes Jaap JansenDocument23 pages2011 Longstanding Adduction-Related Groin Pain in Athletes Jaap JansenJos VreekenNo ratings yet
- Loadin Startle ResponsDocument5 pagesLoadin Startle ResponsramopavelNo ratings yet
- Fukuda 2012 Hip Posterolateral Musculature StreDocument8 pagesFukuda 2012 Hip Posterolateral Musculature StreSebastian RojasNo ratings yet
- Hospital, UK: B-16 Analysis of Knee Kinematics With Computer NavigationDocument1 pageHospital, UK: B-16 Analysis of Knee Kinematics With Computer NavigationMaria BrehaNo ratings yet
- Aging of The Postural VerticalDocument10 pagesAging of The Postural VerticalViolant Verges ForesNo ratings yet
- 26 - Jpts 2013 409Document3 pages26 - Jpts 2013 409merdemerdemerde92No ratings yet
- Lumbar Kinematic Variability During Gait in Chronic Low Back Pain and Associations With Pain, Disability and Isolated Lumbar Extension StrengthDocument8 pagesLumbar Kinematic Variability During Gait in Chronic Low Back Pain and Associations With Pain, Disability and Isolated Lumbar Extension StrengthebiNo ratings yet
- Saeterbakken2013 PDFDocument8 pagesSaeterbakken2013 PDFArthur MendozaNo ratings yet
- (En) Dor Lombar e Mobilidade Renal - A Manipulação Osteopática Fascial Local Diminui A Percepção Da Dor e Melhora A Mobilidade RenalDocument11 pages(En) Dor Lombar e Mobilidade Renal - A Manipulação Osteopática Fascial Local Diminui A Percepção Da Dor e Melhora A Mobilidade RenalCueioNo ratings yet
- Physical Therapy in Sport: Original ResearchDocument6 pagesPhysical Therapy in Sport: Original ResearchErick Andrade IbarraNo ratings yet
- Bru Magne 2004Document4 pagesBru Magne 2004Juan PalomoNo ratings yet
- Vicenzino Keynote1 MUllConf09Document56 pagesVicenzino Keynote1 MUllConf09agniosaiNo ratings yet
- Relationship Between Urethral and Vaginal Pressures During Pelvic Muscle ContractionDocument2 pagesRelationship Between Urethral and Vaginal Pressures During Pelvic Muscle Contractionverica jankelicNo ratings yet
- Surgical Outcomes of Additional Posterior Lumbar Interbody Fusion For Adjacent Segment Disease After Single-Level Posterior Lumbar Interbody FusionDocument5 pagesSurgical Outcomes of Additional Posterior Lumbar Interbody Fusion For Adjacent Segment Disease After Single-Level Posterior Lumbar Interbody FusionwilsonwqaNo ratings yet
- Di GiorgioDocument5 pagesDi GiorgiodiegomosqueracanosaNo ratings yet
- 45 Achilles Tendon Rupt 2018 Clinical Orthopaedic Rehabilitation A Team ADocument5 pages45 Achilles Tendon Rupt 2018 Clinical Orthopaedic Rehabilitation A Team AJessica HongNo ratings yet
- Lisica Lucija-08.04.Document7 pagesLisica Lucija-08.04.Ivan PerićNo ratings yet
- Pelzer Et Al., 2017 - Periodization Effects During Short-Term Resistance Training With Equated Exercise Variables in FemalesDocument14 pagesPelzer Et Al., 2017 - Periodization Effects During Short-Term Resistance Training With Equated Exercise Variables in FemalesRicardo Pereira NevesNo ratings yet
- Effect of Expertise and Visual Contribution On Postural Control in SoccerDocument4 pagesEffect of Expertise and Visual Contribution On Postural Control in Soccernico Michou-SaucetNo ratings yet
- 1997 Effects of Corrective Taping of The Patella On Patients With Patellofemoral PainDocument7 pages1997 Effects of Corrective Taping of The Patella On Patients With Patellofemoral PainWei HungNo ratings yet
- The Effect of Forefoot Varus On Postural StabilityDocument7 pagesThe Effect of Forefoot Varus On Postural Stabilitychungkailun1No ratings yet
- Chronobiology of Labour Pain Perception: An Observational StudyDocument3 pagesChronobiology of Labour Pain Perception: An Observational StudydrszigetilearnNo ratings yet
- Acute Effect of Eccentric Overload Exercises On.8Document7 pagesAcute Effect of Eccentric Overload Exercises On.8Jorge Rubio LopezNo ratings yet
- Brenneman 2016Document9 pagesBrenneman 2016VALENNo ratings yet
- Echilibru - VedereDocument17 pagesEchilibru - VedereEliMihaelaNo ratings yet
- Amiaz 2021 Responses To Balance Challenges in Persons With Panic Disorder A Pilot Study ofDocument12 pagesAmiaz 2021 Responses To Balance Challenges in Persons With Panic Disorder A Pilot Study ofJuan Hernández GarcíaNo ratings yet
- Alterations in Mechanical Properties of The Patellar Tendon Is Associated With Pain in Athletes With Patellar TendinopathyDocument7 pagesAlterations in Mechanical Properties of The Patellar Tendon Is Associated With Pain in Athletes With Patellar TendinopathyIsrael Oña CisnerosNo ratings yet
- Analysis of Hip Strength in Females Seeking Physical Therapy Treatment For Unilateral PFPDocument7 pagesAnalysis of Hip Strength in Females Seeking Physical Therapy Treatment For Unilateral PFPg499bqps5nNo ratings yet
- Influence of KinesiofobiaDocument6 pagesInfluence of KinesiofobiaJamaica MoscosoNo ratings yet
- 1430 2863 1 SMDocument29 pages1430 2863 1 SMsintaNo ratings yet
- Posturañl Sway Change During Pregnancy A Descriptive Study Using StabilometryDocument4 pagesPosturañl Sway Change During Pregnancy A Descriptive Study Using StabilometrySharon BalboaNo ratings yet
- Jurnal Kardio KrisnaDocument10 pagesJurnal Kardio Krisnani made manik gita sanjiwaniNo ratings yet
- Farahpour 2016Document6 pagesFarahpour 2016AbdoulOlaNo ratings yet
- Clinical Biomechanics: Thomas J. Kibsgård, Olav Røise, Bengt Sturesson, Stephan M. Röhrl, Britt StugeDocument6 pagesClinical Biomechanics: Thomas J. Kibsgård, Olav Røise, Bengt Sturesson, Stephan M. Röhrl, Britt StugeLuis HerreraNo ratings yet
- Cervical Spine Hyperextension and Altered Posturo-Respiratory Coupling in Patients With Obstructive Sleep Apnea SyndromeDocument10 pagesCervical Spine Hyperextension and Altered Posturo-Respiratory Coupling in Patients With Obstructive Sleep Apnea SyndromeDenise MathreNo ratings yet
- 2007 Toumi - New Insights Into The Function of The VM With Clinical ImplicationsDocument7 pages2007 Toumi - New Insights Into The Function of The VM With Clinical ImplicationsGabriel BeloNo ratings yet
- Developmental Binocular Vision AbnormalitiesDocument10 pagesDevelopmental Binocular Vision AbnormalitiesGian Carlo Giusto BurboaNo ratings yet
- Vestibular and Proprioceptive Contributions To Human Balance CorrectionsDocument12 pagesVestibular and Proprioceptive Contributions To Human Balance CorrectionsGinaDyoSalsabilaNo ratings yet
- Acupunct Med-2010-Freire-115-9Document6 pagesAcupunct Med-2010-Freire-115-9LA RESONANCIA MÓRFICANo ratings yet
- Jurnal Neuro 6Document7 pagesJurnal Neuro 6ringgoNo ratings yet
- Patients With Patellofemoral Pain Have Lower SoftDocument7 pagesPatients With Patellofemoral Pain Have Lower SofturosNo ratings yet
- Pelvic Inflammatory Disease: Group Members Nancy Nisha Mohammed Aathif.ADocument7 pagesPelvic Inflammatory Disease: Group Members Nancy Nisha Mohammed Aathif.AcindyNo ratings yet
- Tutorial 8 Cardiac ExamDocument14 pagesTutorial 8 Cardiac Examcindy100% (1)
- Intoeing: What Are The Major Causes: 1. Metatarsus Adductus: Seen in First Couple of Months of Age. The Front PartDocument2 pagesIntoeing: What Are The Major Causes: 1. Metatarsus Adductus: Seen in First Couple of Months of Age. The Front PartcindyNo ratings yet
- Assignment-1 ICMDocument2 pagesAssignment-1 ICMcindyNo ratings yet
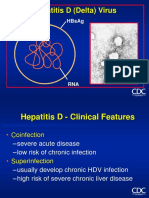
- Hepatitis D (Delta) Virus: Hbsag AntigenDocument6 pagesHepatitis D (Delta) Virus: Hbsag AntigencindyNo ratings yet
- Pulse Oximetry Submitted by Sabarivasan Velsamy Md3B: Oxygen SaturationDocument3 pagesPulse Oximetry Submitted by Sabarivasan Velsamy Md3B: Oxygen SaturationcindyNo ratings yet
- Texila American University: Article Review GuidelineDocument10 pagesTexila American University: Article Review GuidelinecindyNo ratings yet
- Medical Embryology Assignment-1Document10 pagesMedical Embryology Assignment-1cindyNo ratings yet
- Human Chromosomal AbnormalitiesDocument3 pagesHuman Chromosomal Abnormalitiescindy0% (1)
- Case StudyDocument8 pagesCase Studycindy100% (1)
- Pork TocinoDocument1 pagePork TocinoMaria Ivz ElborNo ratings yet
- Essays: 1-Title: Physical FitnessDocument7 pagesEssays: 1-Title: Physical FitnessMy PcNo ratings yet
- 23 Medicinal Plants The Native Americans Used On A Daily Basis - MSYCDocument15 pages23 Medicinal Plants The Native Americans Used On A Daily Basis - MSYCLeandro RodriguesNo ratings yet
- Summary Report On Health and HygieneDocument4 pagesSummary Report On Health and HygieneVisal ShresthaNo ratings yet
- Secondary P.E. 10 Q3Document9 pagesSecondary P.E. 10 Q3Jayzi VicenteNo ratings yet
- Wiley Veterinary GynaecologyDocument2 pagesWiley Veterinary Gynaecologysanath0% (1)
- Osteoarthritis of The Hip and Knee Flowchart PDFDocument2 pagesOsteoarthritis of The Hip and Knee Flowchart PDFsilkofosNo ratings yet
- RLE Module 3F Course Module and Procedure Guide 2Document7 pagesRLE Module 3F Course Module and Procedure Guide 2KaiNo ratings yet
- Dapus FixDocument2 pagesDapus FixIkrima MuhdarmuhallyNo ratings yet
- Experiment NoDocument3 pagesExperiment NoMaxene Kaye PeñaflorNo ratings yet
- HSG 9 Hà Tĩnh 2021Document6 pagesHSG 9 Hà Tĩnh 2021Cachi100% (1)
- Fluid Overload and Kidney Injury Score As A PredicDocument7 pagesFluid Overload and Kidney Injury Score As A Predicmira srikandiNo ratings yet
- Acetylsalicylic AcidDocument6 pagesAcetylsalicylic AcidAdmin DownloadNo ratings yet
- Project Proposal: A. Project Tittle: "Operation Cleanliness"Document8 pagesProject Proposal: A. Project Tittle: "Operation Cleanliness"Mike Avila100% (1)
- Darrells ResumeDocument5 pagesDarrells Resumeapi-273253154No ratings yet
- Phil Airlines v. NLRCDocument1 pagePhil Airlines v. NLRCAlec VenturaNo ratings yet
- TimoDocument9 pagesTimopbchantaNo ratings yet
- Organ SystemsDocument2 pagesOrgan SystemsArnel LaspinasNo ratings yet
- Ma 00507c Us KXL BrochureDocument8 pagesMa 00507c Us KXL BrochureEng. Rijulesh KaremmalNo ratings yet
- Platelet Analysis - An Overview: HistoryDocument7 pagesPlatelet Analysis - An Overview: HistoryPieter Du Toit-EnslinNo ratings yet
- School Nutritional Status Record: Grade 7 - JoyDocument4 pagesSchool Nutritional Status Record: Grade 7 - JoySidNo ratings yet
- Physical Examination FormDocument4 pagesPhysical Examination FormDawit KumsaNo ratings yet
- Effectiveness of Maitland vs. Mulligan Mobilization Techniques in (Ingles)Document4 pagesEffectiveness of Maitland vs. Mulligan Mobilization Techniques in (Ingles)mauricio castroNo ratings yet
- Nursing Care Plan: Phinma University of PangasinanDocument1 pageNursing Care Plan: Phinma University of PangasinanShaira De La CruzNo ratings yet