You might also like
- Herman Gendered Restrooms and Minority Stress June 2013Document16 pagesHerman Gendered Restrooms and Minority Stress June 2013Julisa FernandezNo ratings yet
- Nursing Diagnoses in Psyciatric PDFDocument734 pagesNursing Diagnoses in Psyciatric PDFEgi MunandarNo ratings yet
- Nursing Diagnoses in Psyciatric PDFDocument734 pagesNursing Diagnoses in Psyciatric PDFEgi MunandarNo ratings yet
- Campus Sexual Violence - Statistics - RAINNDocument6 pagesCampus Sexual Violence - Statistics - RAINNJulisa FernandezNo ratings yet
- Oral Presentation Nursing CareerDocument14 pagesOral Presentation Nursing CareerJulisa FernandezNo ratings yet
- Child Abuse Likelier at Church Than Transgender BathroomDocument11 pagesChild Abuse Likelier at Church Than Transgender BathroomJulisa FernandezNo ratings yet
- Hands Only CPRDocument7 pagesHands Only CPRJulisa FernandezNo ratings yet
- Drug Dosage and IV Rates Calculations PDFDocument6 pagesDrug Dosage and IV Rates Calculations PDFvarmaNo ratings yet
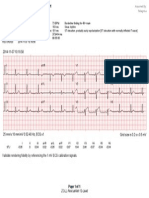
- Validate Rendering Fidelity by Referencing The 1 MV ECG Calibration SignalsDocument1 pageValidate Rendering Fidelity by Referencing The 1 MV ECG Calibration SignalsJulisa FernandezNo ratings yet
- Ecg PediaDocument2 pagesEcg PediaAdrian Ulu100% (1)
- Terapia de Oxigeno en EmsDocument12 pagesTerapia de Oxigeno en EmsJulisa FernandezNo ratings yet
- Drug Dosage and IV Rates Calculations PDFDocument6 pagesDrug Dosage and IV Rates Calculations PDFvarmaNo ratings yet
- Dosage CalculationsDocument39 pagesDosage Calculationssalak9462900% (1)
- Ecg in Emergency Medicine and Acute Care-2005Document420 pagesEcg in Emergency Medicine and Acute Care-2005Ioana Nicoleta Dinu91% (22)
- Clinical Calculation 5 Edition: Pediatric Dosage Pages 211 - 232Document15 pagesClinical Calculation 5 Edition: Pediatric Dosage Pages 211 - 232Adrianus NyomanNo ratings yet
- Dosage CalculationsDocument39 pagesDosage Calculationssalak9462900% (1)
- Guia Itls Septima EdicionDocument396 pagesGuia Itls Septima EdicionJulisa Fernandez100% (1)
- The Nursing Student's Practical Guide To Writing Care Plans by Luanne BeginDocument67 pagesThe Nursing Student's Practical Guide To Writing Care Plans by Luanne Beginsoghosa100% (1)
- Drug Dosage and IV Rates Calculations PDFDocument6 pagesDrug Dosage and IV Rates Calculations PDFvarmaNo ratings yet
- Technical Search Considerations - Listening TechniquesDocument41 pagesTechnical Search Considerations - Listening TechniquesJulisa FernandezNo ratings yet
- Disrythmia Recognition ACLS ASHIDocument127 pagesDisrythmia Recognition ACLS ASHIJulisa FernandezNo ratings yet
- Teaching Resource For Instructors inDocument987 pagesTeaching Resource For Instructors inJulisa FernandezNo ratings yet
- PediatricResuscMeds HOPUDocument1 pagePediatricResuscMeds HOPUJulisa FernandezNo ratings yet
- Part 2. Planning of Major IncidentsDocument53 pagesPart 2. Planning of Major IncidentsJulisa FernandezNo ratings yet
- Technical Search Considerations - Search MarkingsDocument24 pagesTechnical Search Considerations - Search MarkingsJulisa FernandezNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Bedtime Stories 01 Sri Guru Gobind Singh Ji by Santokh Singh Jagdev PDFDocument80 pagesBedtime Stories 01 Sri Guru Gobind Singh Ji by Santokh Singh Jagdev PDFDr. Kamalroop Singh100% (1)
- Ifakara Position AnnouncementDocument2 pagesIfakara Position AnnouncementRashid BumarwaNo ratings yet
- Eligible Candidates List For MD MS Course CLC Round 2 DME PG Counselling 2023Document33 pagesEligible Candidates List For MD MS Course CLC Round 2 DME PG Counselling 2023Dr. Vishal SengarNo ratings yet
- MTB - 1 - LP Q1 W4-Letter TTDocument42 pagesMTB - 1 - LP Q1 W4-Letter TTMasher ViosNo ratings yet
- Front Page.20Document24 pagesFront Page.20Nawshad AhmedNo ratings yet
- BTEC Unit Description GT1F3 v3Document7 pagesBTEC Unit Description GT1F3 v3Fawaaz KhurwolahNo ratings yet
- Chapter 2 Lesson 1 NCBTS and PPSTDocument32 pagesChapter 2 Lesson 1 NCBTS and PPSTMichael CabangonNo ratings yet
- LKG Syllabus 2020Document5 pagesLKG Syllabus 2020wasim bariNo ratings yet
- Impact of OC and LeadershipDocument8 pagesImpact of OC and Leadershiperrytrina putriNo ratings yet
- Mediating The MessageDocument322 pagesMediating The MessageAnda Vanesky100% (2)
- 1 Evaluation of Buildings in Real Conditions of Use - Current SituationDocument11 pages1 Evaluation of Buildings in Real Conditions of Use - Current Situationhaniskamis82No ratings yet
- ESU Is Targeted at Students Identified by Schools To Be at Risk of Dropping Out of School and Those Who Have Dropped Out of SchoolsDocument3 pagesESU Is Targeted at Students Identified by Schools To Be at Risk of Dropping Out of School and Those Who Have Dropped Out of SchoolsYuan ZhenNo ratings yet
- Building High Performance Teams Stages of Team Development Characteristics of A High Performing Team Benefits of A High Performing TeamDocument12 pagesBuilding High Performance Teams Stages of Team Development Characteristics of A High Performing Team Benefits of A High Performing TeamKezie0303No ratings yet
- Final Exam b2 Answer SheetDocument2 pagesFinal Exam b2 Answer SheetTolga ÖzcanNo ratings yet
- Individual & SocietyDocument7 pagesIndividual & SocietyVictor Xavi Lor0% (1)
- Spacehandbook 20180418 Web PDFDocument24 pagesSpacehandbook 20180418 Web PDFMizta HariNo ratings yet
- Weekly Home Learning Plan Grade 6-Justice: Schools Division of Misamis Oriental Kimaya Integrated SchoolDocument16 pagesWeekly Home Learning Plan Grade 6-Justice: Schools Division of Misamis Oriental Kimaya Integrated SchoolDaling JessaNo ratings yet
- Year 5daily Lesson Plans Success Criteria Pupils Can 1. Listen and Underline 4 Correct Words. 2. Read and Fill in at Least 6 Blanks CorrectlyDocument8 pagesYear 5daily Lesson Plans Success Criteria Pupils Can 1. Listen and Underline 4 Correct Words. 2. Read and Fill in at Least 6 Blanks Correctlyjulie ayobNo ratings yet
- Worksheet No. 4.1A Detailed Lesson Plan in Eim T. V. L.: I. ObjectivesDocument3 pagesWorksheet No. 4.1A Detailed Lesson Plan in Eim T. V. L.: I. Objectivesramel gedorNo ratings yet
- Cross Cultural Understanding 03 CultureDocument11 pagesCross Cultural Understanding 03 Cultureestu kaniraNo ratings yet
- Week 1 The Scientific Method of ResearchDocument12 pagesWeek 1 The Scientific Method of ResearchJia Jun VooNo ratings yet
- Review: A. Read and Choose The Correct OptionDocument2 pagesReview: A. Read and Choose The Correct OptionJuan GonzalezNo ratings yet
- Esl Siop SpanishDocument2 pagesEsl Siop Spanishapi-246223007100% (2)
- Babcock - Student Application SANDRA NWENEDocument2 pagesBabcock - Student Application SANDRA NWENEnwenes5258No ratings yet
- Health Equity: Ron Chapman, MD, MPH Director and State Health Officer California Department of Public HealthDocument20 pagesHealth Equity: Ron Chapman, MD, MPH Director and State Health Officer California Department of Public HealthjudemcNo ratings yet
- Philosophy of Social Science:: A Cheat Sheet For Understanding The World Ontology:: Is There A Reality That I Can Know Stuff About?Document3 pagesPhilosophy of Social Science:: A Cheat Sheet For Understanding The World Ontology:: Is There A Reality That I Can Know Stuff About?BangledangleNo ratings yet
- Course Syllabus - Cooking Theory Sept09Document20 pagesCourse Syllabus - Cooking Theory Sept09jermsemail0204No ratings yet
- ПисьмаDocument74 pagesПисьмаAngelina IvanskayaNo ratings yet
- Inverse VariationDocument4 pagesInverse VariationSiti Ida MadihaNo ratings yet
- The Age of Reform (1820 - 1860)Document25 pagesThe Age of Reform (1820 - 1860)Froilan TinduganNo ratings yet