You might also like
- Atrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesFrom EverandAtrial Fibrillation A Simple Guide to The Condition, Treatment And Related DiseasesRating: 4 out of 5 stars4/5 (1)
- Antihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityDocument71 pagesAntihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityMoonAIRNo ratings yet
- Antihypertensive AgentsDocument41 pagesAntihypertensive AgentsRwapembe StephenNo ratings yet
- NAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)From EverandNAPLEX Practice Question Workbook: 1,000+ Comprehensive Practice Questions (2023 Edition)Rating: 4.5 out of 5 stars4.5/5 (3)
- Hypertension TejaDocument64 pagesHypertension TejaAnushka MaheshwariNo ratings yet
- Lec 22 ANTIHYPERTENSIVE - 2Document22 pagesLec 22 ANTIHYPERTENSIVE - 2Abdul MananNo ratings yet
- Cardiovascular Endocrinology and Metabolism: Theory and Practice of Cardiometabolic MedicineFrom EverandCardiovascular Endocrinology and Metabolism: Theory and Practice of Cardiometabolic MedicineAndrew J. KrentzNo ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- Anti Hypertensive DrugsDocument46 pagesAnti Hypertensive DrugsShabaka KashataNo ratings yet
- Anti Hypertensive 20191211Document35 pagesAnti Hypertensive 20191211helloitsmenadNo ratings yet
- 10 and 11 Treatment of Hypertension and AnginaDocument10 pages10 and 11 Treatment of Hypertension and AnginaBrandon AviciiNo ratings yet
- Anti-hypertensive Drugs GuideDocument16 pagesAnti-hypertensive Drugs GuideALNAKINo ratings yet
- HTN JmiDocument39 pagesHTN Jmink999999No ratings yet
- Cardiology Review: HTN: Julia Akaah M.DDocument40 pagesCardiology Review: HTN: Julia Akaah M.DJose LunaNo ratings yet
- Essential Guidelines for Managing HypertensionDocument23 pagesEssential Guidelines for Managing HypertensionMaulana HasanNo ratings yet
- Antinanginal DrugsDocument43 pagesAntinanginal DrugsHUZAIFA YAMAANNo ratings yet
- ANTIHYPERTENSIVE DRUGS: DIURETICS, BETA-BLOCKERS, ACE INHIBITORSDocument37 pagesANTIHYPERTENSIVE DRUGS: DIURETICS, BETA-BLOCKERS, ACE INHIBITORSIrna Purwanti RahayuNo ratings yet
- Ishac M2 Cardio Antihypertensives 2010Document16 pagesIshac M2 Cardio Antihypertensives 2010Franchesca LugoNo ratings yet
- HypertensionDocument54 pagesHypertensionBadri KarkiNo ratings yet
- Antihypertensive & Antianginal DrugsDocument5 pagesAntihypertensive & Antianginal Drugsdomememe1No ratings yet
- 7,8 - Antihypertensive DrugsDocument10 pages7,8 - Antihypertensive DrugsHusniya MehamedNo ratings yet
- Antihypertensive Drugs.Document35 pagesAntihypertensive Drugs.Abdul WahabNo ratings yet
- Antihypertensive Drugs ٠١١٦٥٨Document10 pagesAntihypertensive Drugs ٠١١٦٥٨mohnad806mNo ratings yet
- Antihypertensive Agents GuideDocument3 pagesAntihypertensive Agents GuideCharles BayogNo ratings yet
- FARMAKOGNOSI - Obat AntihipertensiDocument7 pagesFARMAKOGNOSI - Obat AntihipertensiTrianisa FebyNo ratings yet
- 1 Antihypertensive DrugsDocument14 pages1 Antihypertensive DrugsReda SoNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- Hypertension PDFDocument57 pagesHypertension PDFrahul m dNo ratings yet
- Antihypertensive DrugsDocument7 pagesAntihypertensive Drugshamadadodo7No ratings yet
- Cholinergic System: e CarbamatesDocument26 pagesCholinergic System: e CarbamatesAcai BoncaiNo ratings yet
- Anti-Hypertensive Drugs Classification and MechanismsDocument64 pagesAnti-Hypertensive Drugs Classification and MechanismsPSC100% (1)
- Antihypertensive AgentsDocument52 pagesAntihypertensive Agentssameena ramzanNo ratings yet
- Class: Statin (PCKS9 Inhibitors) o High Intensity: Atorvastatin (Lipitor), Rosuvastatin (Crestor)Document15 pagesClass: Statin (PCKS9 Inhibitors) o High Intensity: Atorvastatin (Lipitor), Rosuvastatin (Crestor)LionelWrightNo ratings yet
- Study Guide For Final Pharmacology HypertensionDocument39 pagesStudy Guide For Final Pharmacology HypertensionAlejandro Daniel Landa MoralesNo ratings yet
- Anti-Anginal Drugs ExplainedDocument19 pagesAnti-Anginal Drugs ExplainedAnusha ZubairNo ratings yet
- Antihypertensive Drugs: Loretta Walker, PH.DDocument11 pagesAntihypertensive Drugs: Loretta Walker, PH.DAdrian Jake LiuNo ratings yet
- Antihypertensive Drugs: HypertensionDocument8 pagesAntihypertensive Drugs: Hypertensionalmastar officeNo ratings yet
- Sympatholytic DrugsDocument20 pagesSympatholytic DrugsAudrey Beatrice Reyes100% (1)
- 11A Drugs Acting On The Cardiovascular SystemDocument85 pages11A Drugs Acting On The Cardiovascular SystemJaps De la CruzNo ratings yet
- AntiHypertensives (Autosaved)Document64 pagesAntiHypertensives (Autosaved)UsamaNo ratings yet
- CHF Drugs Guide: Key Medications for Treating Congestive Heart FailureDocument21 pagesCHF Drugs Guide: Key Medications for Treating Congestive Heart Failuremohsen mirdamadiNo ratings yet
- Anti Hypertensives Overvi-35247Document40 pagesAnti Hypertensives Overvi-35247Alben SigamaniNo ratings yet
- Anti Hypertensive DrugsDocument9 pagesAnti Hypertensive DrugsBaqir BroNo ratings yet
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Hypertension An OverviewDocument214 pagesHypertension An OverviewdkhandkeNo ratings yet
- Cvs DrugsDocument106 pagesCvs DrugsIkoona ivanNo ratings yet
- CVD and HTNDocument60 pagesCVD and HTNZsazsa100% (1)
- Lecture 24-25 - Antihypertensive AgentsDocument30 pagesLecture 24-25 - Antihypertensive AgentsJedoNo ratings yet
- M. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersDocument21 pagesM. Gabriel Khan - Cardiac Drug Therapy, Calcium Channel BlockersluongcongthucNo ratings yet
- Congestive Heart Failure: CardiacDocument36 pagesCongestive Heart Failure: CardiacHUZAIFA YAMAANNo ratings yet
- Adrenergic Antagonists: An Introduction to Alpha and Beta BlockersDocument64 pagesAdrenergic Antagonists: An Introduction to Alpha and Beta BlockersAneeza AhmadNo ratings yet
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocument5 pagesPharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SNo ratings yet
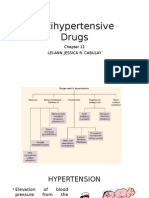
- Antihypertensive DrugsDocument37 pagesAntihypertensive Drugsleiann_jessicaNo ratings yet
- Dr Bahram Soltan - Hypertension Mechanisms and TreatmentDocument64 pagesDr Bahram Soltan - Hypertension Mechanisms and TreatmentParsa EbrahimpourNo ratings yet
- CVPR Prototype Drugs TableDocument27 pagesCVPR Prototype Drugs TablethommyvaNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- 3.07 AntiHypertensive Drugs, COMJ, 2022Document35 pages3.07 AntiHypertensive Drugs, COMJ, 2022JedoNo ratings yet
- LeprosyDocument27 pagesLeprosyAiman TymerNo ratings yet
- MycosesDocument28 pagesMycosesAiman TymerNo ratings yet
- PYODERMADocument45 pagesPYODERMAAiman Tymer80% (5)
- Pyoderma (Derma Presentation)Document11 pagesPyoderma (Derma Presentation)Aiman Tymer100% (1)
- Lupus ErythematosusDocument7 pagesLupus ErythematosusAiman TymerNo ratings yet
- Psy Exam 5th Year PDFDocument47 pagesPsy Exam 5th Year PDFAiman TymerNo ratings yet
- Neuro DermatitisDocument19 pagesNeuro DermatitisAiman Tymer100% (1)
- EczemaDocument19 pagesEczemaAiman TymerNo ratings yet
- Echzema DermatitisDocument7 pagesEchzema DermatitisAiman TymerNo ratings yet
- SclerodermaDocument36 pagesSclerodermaAiman TymerNo ratings yet
- SclerodermaDocument9 pagesSclerodermaAiman TymerNo ratings yet
- Dermatology Lupus Erythematosus: Name: Muhammad Nooraiman Ahmad Noordin Group: 30 ADocument14 pagesDermatology Lupus Erythematosus: Name: Muhammad Nooraiman Ahmad Noordin Group: 30 AAiman TymerNo ratings yet
- Genital Herpes: Aarthi (2012)Document36 pagesGenital Herpes: Aarthi (2012)Aiman TymerNo ratings yet
- Viral Hepatitis: by Shalini Hazael, Group 40aDocument24 pagesViral Hepatitis: by Shalini Hazael, Group 40aAiman TymerNo ratings yet
- Chlamydia: Harsheni Chandran 40 ADocument13 pagesChlamydia: Harsheni Chandran 40 AAiman TymerNo ratings yet
- Genital Herpes: Aarthi (2012)Document36 pagesGenital Herpes: Aarthi (2012)Aiman TymerNo ratings yet
- Donovanosis (Granuloma Inguinale) .PpsDocument14 pagesDonovanosis (Granuloma Inguinale) .PpsAiman TymerNo ratings yet
- Diagnostics of SyphilisDocument18 pagesDiagnostics of SyphilisAiman TymerNo ratings yet
- Donovanosis (Granuloma Inguinale) .PpsDocument14 pagesDonovanosis (Granuloma Inguinale) .PpsAiman TymerNo ratings yet
- Yaw (Tropical Syphilis)Document16 pagesYaw (Tropical Syphilis)Aiman Tymer100% (1)
- Blood Normal TableDocument1 pageBlood Normal TableAiman TymerNo ratings yet
- Pinta (Tropical Syphilis)Document17 pagesPinta (Tropical Syphilis)Aiman Tymer100% (1)
- Test Surgery Exam (Eng)Document36 pagesTest Surgery Exam (Eng)Aiman TymerNo ratings yet
- Micro Sample Patan ExamDocument15 pagesMicro Sample Patan ExamAiman TymerNo ratings yet
- Surgery Examination - 3-4 (Question Cases) (Eng)Document45 pagesSurgery Examination - 3-4 (Question Cases) (Eng)Aiman TymerNo ratings yet
- Dermatology Scleroderma: Click To Edit Master Subtitle StyleDocument36 pagesDermatology Scleroderma: Click To Edit Master Subtitle StyleAiman Tymer100% (1)
- Macro Sample Pathan ExamDocument17 pagesMacro Sample Pathan ExamAiman TymerNo ratings yet
- LeprosyDocument27 pagesLeprosyAiman TymerNo ratings yet
- Dermatology Eczema: Click To Edit Master Subtitle StyleDocument19 pagesDermatology Eczema: Click To Edit Master Subtitle StyleAiman Tymer100% (1)
- BBL™ Mueller Hinton Broth: - Rev. 02 - June 2012Document2 pagesBBL™ Mueller Hinton Broth: - Rev. 02 - June 2012Manam SiddiquiNo ratings yet
- A 55-Year-Old Woman With Shock and Labile Blood PressureDocument11 pagesA 55-Year-Old Woman With Shock and Labile Blood PressureMr. LNo ratings yet
- Congenital SyphilisDocument28 pagesCongenital SyphilisMeena Koushal100% (4)
- 2018 Overview Digestive System HandoutDocument11 pages2018 Overview Digestive System HandoutdraganNo ratings yet
- Nursing Care Plan Neonatal PneumoniaDocument2 pagesNursing Care Plan Neonatal Pneumoniaderic93% (41)
- WORKSHEET 3 Lymphocyte ActivationDocument5 pagesWORKSHEET 3 Lymphocyte ActivationNeha ChoudharyNo ratings yet
- New Drugs 2014-2018Document31 pagesNew Drugs 2014-2018Prem Goel0% (1)
- Nursing Diagnosis For AsthmaDocument6 pagesNursing Diagnosis For AsthmaTINAIDA33% (3)
- 03 Biosecurity Jit PPT FinalDocument20 pages03 Biosecurity Jit PPT FinalReza WratsongkoNo ratings yet
- Pneumonia: Causes, Signs, Symptoms and Nursing CareDocument16 pagesPneumonia: Causes, Signs, Symptoms and Nursing CareMelissa David100% (1)
- Salivation PDFDocument5 pagesSalivation PDFmehdi mafakheri100% (1)
- Superannuation Benefits SessionDocument49 pagesSuperannuation Benefits SessionfunshareNo ratings yet
- Scientific Breakthroughs in Autophagy MechanismsDocument7 pagesScientific Breakthroughs in Autophagy MechanismshananNo ratings yet
- Food For The BrainDocument34 pagesFood For The BrainKristine Mae AbrasaldoNo ratings yet
- Acute and Chronic PyelonephritisDocument7 pagesAcute and Chronic PyelonephritisMatthew Ryan100% (1)
- Indian Herbs Cooking GuideDocument37 pagesIndian Herbs Cooking Guidehitesh mendirattaNo ratings yet
- Science Magazine, Issue 6657 (August 4, 2023)Document175 pagesScience Magazine, Issue 6657 (August 4, 2023)Kim LevrelNo ratings yet
- Biochem SGD 3Document4 pagesBiochem SGD 3Hemanth KokaNo ratings yet
- CDC's HIV Infection Through Oral Sex, Fact SheetDocument2 pagesCDC's HIV Infection Through Oral Sex, Fact SheetCésar E. ConcepciónNo ratings yet
- Letter WritingDocument17 pagesLetter WritingEmtiaj RahmanNo ratings yet
- WHATs New in CPCRDocument4 pagesWHATs New in CPCRJessicaHernandezNo ratings yet
- GugulipidDocument7 pagesGugulipidManish WadhwaniNo ratings yet
- Bipolar Depression Diagnosis and Treatment OptionsDocument21 pagesBipolar Depression Diagnosis and Treatment OptionsThuvija DarshiniNo ratings yet
- Sermon On Spirituality & Mental Illness by Rev Laura MancusoDocument12 pagesSermon On Spirituality & Mental Illness by Rev Laura MancusoRev. Laura L. MancusoNo ratings yet
- Introduction of PHCDocument39 pagesIntroduction of PHCIdiris Mohamed100% (1)
- 2023 Summit Program Draft 5 Apr18Document43 pages2023 Summit Program Draft 5 Apr18Raheem KassamNo ratings yet
- ABG AnalysisDocument15 pagesABG AnalysisPabhat Kumar100% (2)
- Section 5 - Students WorksheetDocument4 pagesSection 5 - Students WorksheetEsraa AhmedNo ratings yet
- Physical Paper +1ANNUALDocument5 pagesPhysical Paper +1ANNUALprabhnoorprimeNo ratings yet
- The Circulatory System - Lecture STEMDocument50 pagesThe Circulatory System - Lecture STEMMargeory Calatan100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)