You might also like
- Efa D 10 00228 1Document25 pagesEfa D 10 00228 1AlesNo ratings yet
- Efa D 10 00228 1Document25 pagesEfa D 10 00228 1AlesNo ratings yet
- Efa D 10 00228 1Document25 pagesEfa D 10 00228 1AlesNo ratings yet
- Effect of Grain Size On Mechanical Properties of SteelDocument8 pagesEffect of Grain Size On Mechanical Properties of SteelAlok JhaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cambridge International AS & A Level: Biology 9700/53 May/June 2021Document11 pagesCambridge International AS & A Level: Biology 9700/53 May/June 2021YeNo ratings yet
- Kedah Skema Modul 2 Kimia Paper 2 Trial SPM 2015Document10 pagesKedah Skema Modul 2 Kimia Paper 2 Trial SPM 2015azmibhr100% (1)
- LC MSDocument15 pagesLC MSSriNo ratings yet
- Counter Flow RegenerationDocument8 pagesCounter Flow Regenerationvel muruganNo ratings yet
- 5991-9013EN InfinityLab Poroshell120 PosterDocument1 page5991-9013EN InfinityLab Poroshell120 PosterSupat MuangyotNo ratings yet
- Week 5 - Learning ActivitiesDocument4 pagesWeek 5 - Learning ActivitiesChuchai Isla Y AbadNo ratings yet
- CHEN3009 Final Exam - Example PaperDocument4 pagesCHEN3009 Final Exam - Example PaperRosario QFNo ratings yet
- LAS Gen - Chem2 - MELC - 2 3 - Q4 Week 1Document10 pagesLAS Gen - Chem2 - MELC - 2 3 - Q4 Week 1Bjai MedallaNo ratings yet
- 2190 NID-38eDocument2 pages2190 NID-38eneden olmasınNo ratings yet
- ChemistryDocument4 pagesChemistryTamerlan KudaibergenNo ratings yet
- Atmospheric PollutionDocument2 pagesAtmospheric Pollutionanshvishwakarma674No ratings yet
- Math Sectional 1Document55 pagesMath Sectional 1jsaab2692No ratings yet
- Standard Operating Procedure - OxidizersDocument5 pagesStandard Operating Procedure - OxidizersMishel Mijares100% (1)
- History Nylon 6Document2 pagesHistory Nylon 6Alessio ScarabelliNo ratings yet
- Coating System SelectionDocument23 pagesCoating System SelectionA. FauziNo ratings yet
- O Level Chemistry Practice QuestionsDocument3 pagesO Level Chemistry Practice Questionschong5675% (12)
- DownloadDocument12 pagesDownloadrelax soundNo ratings yet
- Towards Dense Single-Atom Catalysts For Future Automotive ApplicationsDocument13 pagesTowards Dense Single-Atom Catalysts For Future Automotive ApplicationsAdriano Aj-formataçãoNo ratings yet
- MSDS FlexDocument11 pagesMSDS FlexMujahidin HakimNo ratings yet
- A Review: Uses of Gas Chromatography-Mass Spectrometry (GC-MS) Technique For Analysis of Bioactive Natural Compounds of Some PlantsDocument6 pagesA Review: Uses of Gas Chromatography-Mass Spectrometry (GC-MS) Technique For Analysis of Bioactive Natural Compounds of Some Plantsdita kumaraNo ratings yet
- 1 s2.0 S0143749620300865 MainDocument9 pages1 s2.0 S0143749620300865 MainLautaro Teper MarinelliNo ratings yet
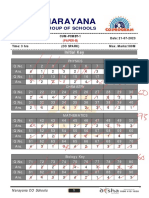
- 7 Sco Cum-Pcmbt-1 (Paper-B) Key Exam DT 21-07-2023Document4 pages7 Sco Cum-Pcmbt-1 (Paper-B) Key Exam DT 21-07-2023Samit KambalapallyNo ratings yet
- Reportsheet#4 Calorimetry Chem1103lDocument6 pagesReportsheet#4 Calorimetry Chem1103lMarielleCaindecNo ratings yet
- Safety Data Sheet AntifreezeDocument8 pagesSafety Data Sheet AntifreezeMithil SawantNo ratings yet
- Fantastic A (Seventh) List of New Mineral Names 2 Mineralogical SocietDocument19 pagesFantastic A (Seventh) List of New Mineral Names 2 Mineralogical SocietLaura BecerraNo ratings yet
- Sigmadur 550 Base WhiteDocument18 pagesSigmadur 550 Base Whitevikram singhNo ratings yet
- Guide For The Use of Polymers in Concrete PDFDocument29 pagesGuide For The Use of Polymers in Concrete PDFMEGA_ONENo ratings yet
- Structured Method Statement For Concrete Repair - 2Document10 pagesStructured Method Statement For Concrete Repair - 2m.umarNo ratings yet
- Injection Moulding Training ManualDocument38 pagesInjection Moulding Training ManualChetan RaoNo ratings yet
- Highly Sensitive and Rugged GC/MS/MS Tool: For Pesticide Multiresidue Analysis in Food SamplesDocument8 pagesHighly Sensitive and Rugged GC/MS/MS Tool: For Pesticide Multiresidue Analysis in Food SamplesDesislav DonchevNo ratings yet