You might also like
- Quality CircleDocument33 pagesQuality CircleSudeesh SudevanNo ratings yet
- Traditional Features of Irish MusicDocument2 pagesTraditional Features of Irish MusicAj Aquino50% (2)
- Introduction To BiopsychosocialDocument30 pagesIntroduction To Biopsychosocialoscar3spurgeon100% (1)
- Rescue Triangle PDFDocument18 pagesRescue Triangle PDFrabas_No ratings yet
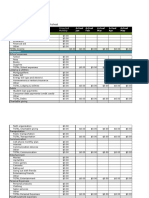
- Masonry Brickwork 230 MMDocument1 pageMasonry Brickwork 230 MMrohanNo ratings yet
- The Biopsychosocial ModelDocument8 pagesThe Biopsychosocial ModelResshaya RoobiniNo ratings yet
- Lesson 1 Introduction To PsychologyDocument8 pagesLesson 1 Introduction To PsychologyMel P. ManaloNo ratings yet
- Adult Nursing Skills On Complex CareDocument16 pagesAdult Nursing Skills On Complex CareNaftali OumaNo ratings yet
- The Biopsychosocial ModelDocument8 pagesThe Biopsychosocial ModelOlaya HernándezNo ratings yet
- MT ReviewerDocument7 pagesMT ReviewerCatherine MerillenoNo ratings yet
- Global 6000 SystemsDocument157 pagesGlobal 6000 SystemsJosé Rezende100% (1)
- 17 Health Behavioral ModelsDocument49 pages17 Health Behavioral ModelsVesley B Robin100% (2)
- Models of DisabilityDocument14 pagesModels of DisabilityMeti Guda100% (1)
- Biological, Social and Biosocial Perspectives On The Formation of Aggression and Violent BehaviourDocument11 pagesBiological, Social and Biosocial Perspectives On The Formation of Aggression and Violent BehaviourChristopher Richard IsaacNo ratings yet
- Biopsychosocial ModelDocument6 pagesBiopsychosocial Modelsamu2-4uNo ratings yet
- Global Consensus on Managing EndometriosisDocument17 pagesGlobal Consensus on Managing EndometriosisCristina BravoNo ratings yet
- Understanding Culture, Society and PoliticsDocument62 pagesUnderstanding Culture, Society and PoliticsTeds TV89% (84)
- Psychotherapy EthicsDocument12 pagesPsychotherapy EthicsPrarthana SagarNo ratings yet
- Biopsychosocial Model Approach PDFDocument2 pagesBiopsychosocial Model Approach PDFJaf BazziNo ratings yet
- Normative Ethics Readings19 20 1Document27 pagesNormative Ethics Readings19 20 1JHUZELL DUMANJOGNo ratings yet
- Psyc3600 Summaries W 1-3Document33 pagesPsyc3600 Summaries W 1-3Kristy Bremmell100% (1)
- Human BehaviourDocument66 pagesHuman Behaviournor hanis100% (1)
- Ethical ApproachesDocument4 pagesEthical ApproachesJustinNo ratings yet
- Health Belief Model - Behavioural ChangeDocument3 pagesHealth Belief Model - Behavioural ChangenieotyagiNo ratings yet
- Reliability and ValidityDocument5 pagesReliability and ValidityMohdzinuri Hasnan100% (1)
- What Is PsychoanalysisDocument5 pagesWhat Is PsychoanalysisNice tuazonNo ratings yet
- Palliative Care Role of NursesDocument5 pagesPalliative Care Role of NursesAj Aquino100% (1)
- Social Influence On ConformityDocument9 pagesSocial Influence On Conformitymonicaherz515No ratings yet
- 3.1 Basic PsychologyDocument23 pages3.1 Basic PsychologyGanesh NaikNo ratings yet
- Diabetic Foot JAAOSDocument8 pagesDiabetic Foot JAAOSAtikah ZuraNo ratings yet
- Sociology of Health and Illness UCSPDocument1 pageSociology of Health and Illness UCSPKarylle YoungNo ratings yet
- Law of ContiguityDocument2 pagesLaw of ContiguityMahmud Abdullahi SarkiNo ratings yet
- Behavioural Approach To AddictionDocument2 pagesBehavioural Approach To AddictionjukazadeNo ratings yet
- EgocentrismDocument20 pagesEgocentrismSuhaili Sobri100% (1)
- Human Growth and DevelopmentDocument14 pagesHuman Growth and DevelopmentAllan SantosNo ratings yet
- Deontological EthicsDocument4 pagesDeontological EthicsNEET ncert readingNo ratings yet
- The Customer Is Not Always RightDocument11 pagesThe Customer Is Not Always RightyaminshaikhNo ratings yet
- 03 Dilemma & 04 Biomedical Ethics Discorse (Prof Hakimi)Document54 pages03 Dilemma & 04 Biomedical Ethics Discorse (Prof Hakimi)Zuzu FinusNo ratings yet
- Personality - Meaning, ConceptDocument15 pagesPersonality - Meaning, ConceptKapil SharmaNo ratings yet
- Egoism: Descriptive vs Normative TheoriesDocument9 pagesEgoism: Descriptive vs Normative TheoriesCeciBohoNo ratings yet
- The Function of Theory Is To Provide Puzzles For Research (Lewis Coser)Document5 pagesThe Function of Theory Is To Provide Puzzles For Research (Lewis Coser)Eduardo Antonio RodríguezNo ratings yet
- Research Paper On HamstersDocument14 pagesResearch Paper On HamstersMalou Eblahan100% (1)
- Research ProposalDocument4 pagesResearch ProposalAmmara Aman100% (1)
- Behavioral System Model by Dorothy JohnsonDocument2 pagesBehavioral System Model by Dorothy JohnsonyoeanneNo ratings yet
- 31 Psychological Defense Mechanisms ExplainedDocument9 pages31 Psychological Defense Mechanisms ExplainedJo Hn Vengz100% (1)
- Defense MechanismDocument19 pagesDefense MechanismmissirenaNo ratings yet
- 4140 Philosophy of NursingDocument10 pages4140 Philosophy of Nursingapi-402049640No ratings yet
- Human Skeleton NotesDocument29 pagesHuman Skeleton NotesSoumyajit DasNo ratings yet
- Using Folktales to Teach Moral Values to StudentsDocument24 pagesUsing Folktales to Teach Moral Values to StudentsMenk JnrNo ratings yet
- Frameworks of EthicsDocument10 pagesFrameworks of EthicsChean SamaniegoNo ratings yet
- George KellyDocument21 pagesGeorge KellyIly IsaNo ratings yet
- Spearman Rank CorrelationDocument18 pagesSpearman Rank CorrelationFia JungNo ratings yet
- Attitudes and Behaviour For TEX3701 2020Document13 pagesAttitudes and Behaviour For TEX3701 2020SleepingPhantomsNo ratings yet
- Lawrence Kohlberg's: Moral Development: Presentation By: Blanco, Leila Cashmire A. Calib-Og, NormanDocument20 pagesLawrence Kohlberg's: Moral Development: Presentation By: Blanco, Leila Cashmire A. Calib-Og, NormanJianna Tang IndingNo ratings yet
- Physiotherapeutic Management of Adhesive Capsulitis Literature ReviewDocument9 pagesPhysiotherapeutic Management of Adhesive Capsulitis Literature ReviewevaNo ratings yet
- Myocardial Infarction MedBack RevisedDocument7 pagesMyocardial Infarction MedBack RevisedSteve ColbertNo ratings yet
- PANRar 16013Document10 pagesPANRar 16013Putu EdyNo ratings yet
- Venous Ulcer: Irene Dorthy Santoso, Hanny Nilasari, Shannaz Nadia YusharyahyaDocument13 pagesVenous Ulcer: Irene Dorthy Santoso, Hanny Nilasari, Shannaz Nadia YusharyahyaIntan CahyaNo ratings yet
- Effect of TENS On Knee OADocument26 pagesEffect of TENS On Knee OAtkrdnawaNo ratings yet
- OsteoartritisDocument11 pagesOsteoartritisSavira Rizka MeidySNo ratings yet
- Obesity Inflammation and Endothelial DysDocument8 pagesObesity Inflammation and Endothelial DysgoldNo ratings yet
- Quality of Life Patients With Ulcus DiabeticDocument4 pagesQuality of Life Patients With Ulcus DiabeticNadiaRashyaNo ratings yet
- Review Article: Diabetic Foot Infections: State-Of-The-ArtDocument13 pagesReview Article: Diabetic Foot Infections: State-Of-The-Artday dayuNo ratings yet
- DP UvDocument3 pagesDP UvAnnisya FitriNo ratings yet
- Rheumatoid Arthritis Thesis PaperDocument6 pagesRheumatoid Arthritis Thesis Paperlauraandersonaurora100% (2)
- Asuhan Keperawatan Keluarga pada Kasus Post StrokeDocument8 pagesAsuhan Keperawatan Keluarga pada Kasus Post StrokeyudhaNo ratings yet
- The Impact of Heart Failure and AgeDocument6 pagesThe Impact of Heart Failure and Ageapi-643186750No ratings yet
- A Strategic Marketing Plan For NikeDocument23 pagesA Strategic Marketing Plan For NikeAj AquinoNo ratings yet
- Discuss The Key Components of Cognitive Behavioural TherapyDocument3 pagesDiscuss The Key Components of Cognitive Behavioural TherapyAj AquinoNo ratings yet
- Original EssayDocument3 pagesOriginal EssayAj AquinoNo ratings yet
- Student Instructions and Guidelines End of Term ExamDocument8 pagesStudent Instructions and Guidelines End of Term ExamAj AquinoNo ratings yet
- Red Oak PackDocument3 pagesRed Oak PackAj AquinoNo ratings yet
- NMHS30970 EBP Workbook 2017-18Document52 pagesNMHS30970 EBP Workbook 2017-18Aj AquinoNo ratings yet
- Alma 32 Seminar Complete TranscriptDocument204 pagesAlma 32 Seminar Complete TranscriptAj AquinoNo ratings yet
- Assessment 3 Template Matrix NMHS30970Document5 pagesAssessment 3 Template Matrix NMHS30970Aj AquinoNo ratings yet
- Congrats on 2nd Tri Win! Westport Tri 2017Document2 pagesCongrats on 2nd Tri Win! Westport Tri 2017Aj AquinoNo ratings yet
- Nursing Diagnosis: Chronic Pain Related To Tissue Distension byDocument4 pagesNursing Diagnosis: Chronic Pain Related To Tissue Distension byAj AquinoNo ratings yet
- Good Morning Brothers and SistersDocument4 pagesGood Morning Brothers and SistersAj AquinoNo ratings yet
- Patient Safety Assignment 2015Document3 pagesPatient Safety Assignment 2015Aj AquinoNo ratings yet
- Irelandss Health Care SystemDocument26 pagesIrelandss Health Care SystemAj AquinoNo ratings yet
- Irelandss Health Care SystemDocument26 pagesIrelandss Health Care SystemAj AquinoNo ratings yet
- Traditional College StudentDocument15 pagesTraditional College StudentAj AquinoNo ratings yet
- PharmDocument1 pagePharmAj AquinoNo ratings yet
- Aaron Beck's CBT & NATsDocument4 pagesAaron Beck's CBT & NATsAj AquinoNo ratings yet
- BBB 2015 Essay BSC Older AdultDocument3 pagesBBB 2015 Essay BSC Older AdultAj AquinoNo ratings yet
- Nursing 8440 Autumn 2012 Grand Theory Presentation 1Document16 pagesNursing 8440 Autumn 2012 Grand Theory Presentation 1Aj AquinoNo ratings yet
- Yin YangDocument2 pagesYin YangAj AquinoNo ratings yet
- 2008 Moral DevelopmentDocument1 page2008 Moral DevelopmentAj AquinoNo ratings yet
- Anatomy Is The Study of The Structure of The Human Body:: Introduction To Anatomy: Anatomical TerminologyDocument9 pagesAnatomy Is The Study of The Structure of The Human Body:: Introduction To Anatomy: Anatomical TerminologyAj AquinoNo ratings yet
- Philip Larkin's Poetry Explores Life's MeaningDocument8 pagesPhilip Larkin's Poetry Explores Life's MeaningAj AquinoNo ratings yet
- The Prevalence of OpenDocument2 pagesThe Prevalence of OpenAj AquinoNo ratings yet
- Yin YangDocument2 pagesYin YangAj AquinoNo ratings yet
- Seachanges With Danse MacacreDocument3 pagesSeachanges With Danse MacacreAj Aquino100% (3)
- SeminaryDocument8 pagesSeminaryAj AquinoNo ratings yet
- Docking 1Document12 pagesDocking 1Naveen Virendra SinghNo ratings yet
- Delhi Public School: Class: XI Subject: Assignment No. 3Document1 pageDelhi Public School: Class: XI Subject: Assignment No. 3Aman Kumar BhagatNo ratings yet
- Flexible AC Transmission SystemsDocument51 pagesFlexible AC Transmission SystemsPriyanka VedulaNo ratings yet
- PGP TutorialDocument21 pagesPGP TutorialSabri AllaniNo ratings yet
- Panasonic TC-P42X5 Service ManualDocument74 pagesPanasonic TC-P42X5 Service ManualManager iDClaimNo ratings yet
- Donaldson 004117 PDFDocument6 pagesDonaldson 004117 PDFNSNo ratings yet
- The Impact of Information Technology and Innovation To Improve Business Performance Through Marketing Capabilities in Online Businesses by Young GenerationsDocument10 pagesThe Impact of Information Technology and Innovation To Improve Business Performance Through Marketing Capabilities in Online Businesses by Young GenerationsLanta KhairunisaNo ratings yet
- CIGB B164 Erosion InterneDocument163 pagesCIGB B164 Erosion InterneJonathan ColeNo ratings yet
- Accidental PoisoningDocument3 pagesAccidental PoisoningBRUELIN MELSHIA MNo ratings yet
- Brooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFDocument36 pagesBrooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFlois.guzman538100% (12)
- Write 10 Lines On My Favourite Subject EnglishDocument1 pageWrite 10 Lines On My Favourite Subject EnglishIrene ThebestNo ratings yet
- EcohistDocument3 pagesEcohistRkmv EconNo ratings yet
- Linguistics: Chapter 1 - 10Document41 pagesLinguistics: Chapter 1 - 10Ahmad A. JawadNo ratings yet
- SuffrageDocument21 pagesSuffragejecelyn mae BaluroNo ratings yet
- Scholars of Hadith Methodology in Dealing With The Two Sahihs: The Criticized Ahadith As A Model. Ammar Ahmad Al-HaririDocument37 pagesScholars of Hadith Methodology in Dealing With The Two Sahihs: The Criticized Ahadith As A Model. Ammar Ahmad Al-HaririSalah KhanNo ratings yet
- Fiery Training 1Document346 pagesFiery Training 1shamilbasayevNo ratings yet
- Estwani ISO CodesDocument9 pagesEstwani ISO Codesनिपुण कुमारNo ratings yet
- Policies and Regulations On EV Charging in India PPT KrishnaDocument9 pagesPolicies and Regulations On EV Charging in India PPT KrishnaSonal ChoudharyNo ratings yet
- Call SANROCCO 11 HappybirthdayBramanteDocument8 pagesCall SANROCCO 11 HappybirthdayBramanterod57No ratings yet
- Zhihua Yao - Dignaga and The 4 Types of Perception (JIP 04)Document24 pagesZhihua Yao - Dignaga and The 4 Types of Perception (JIP 04)Carlos Caicedo-Russi100% (1)
- Febrile SeizureDocument3 pagesFebrile SeizureClyxille GiradoNo ratings yet
- Solr 3000: Special Operations Long Range Oxygen Supply 3,000 PsigDocument2 pagesSolr 3000: Special Operations Long Range Oxygen Supply 3,000 Psigмар'ян коб'ялковськийNo ratings yet
- Universal Robina Co. & Bdo Unibank Inc.: Research PaperDocument25 pagesUniversal Robina Co. & Bdo Unibank Inc.: Research PaperSariephine Grace ArasNo ratings yet
- Eudragit ReviewDocument16 pagesEudragit ReviewlichenresearchNo ratings yet
- HP 5973 Quick ReferenceDocument28 pagesHP 5973 Quick ReferenceDavid ruizNo ratings yet