You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Clinical Characteristics of Pulmonary Embolism With Underlying MalignancyDocument5 pagesClinical Characteristics of Pulmonary Embolism With Underlying MalignancyKaren PinemNo ratings yet
- Goldenhar Syndrome - A Literature Review: JSM DentistryDocument4 pagesGoldenhar Syndrome - A Literature Review: JSM DentistryKaren PinemNo ratings yet
- No CM Nama Umur/ JK Diagnosa Utama Tindakan Sub Bag RuangDocument2 pagesNo CM Nama Umur/ JK Diagnosa Utama Tindakan Sub Bag RuangKaren PinemNo ratings yet
- Nama/Usia/Cm Ruang MRS DPJP Diagnosa Post Tindakan Rencana KeteranganDocument1 pageNama/Usia/Cm Ruang MRS DPJP Diagnosa Post Tindakan Rencana KeteranganKaren PinemNo ratings yet
- Brain Edema in Brain Tumour PDFDocument8 pagesBrain Edema in Brain Tumour PDFKaren PinemNo ratings yet
- Wound Management of Venous Leg Ulcer, Hartmann, 2006Document47 pagesWound Management of Venous Leg Ulcer, Hartmann, 2006Karen PinemNo ratings yet
- Pasien Igd Bedah Rabu, 05/07/2017 Dr. Jaga:Dto/Syh/Ash/Mbu/Kp/Dk/Put No. CM Nama Umur/Jk Diagnosisutama Tindakan Sub Bagian RuangDocument2 pagesPasien Igd Bedah Rabu, 05/07/2017 Dr. Jaga:Dto/Syh/Ash/Mbu/Kp/Dk/Put No. CM Nama Umur/Jk Diagnosisutama Tindakan Sub Bagian RuangKaren PinemNo ratings yet
- 2007 Article 9012Document5 pages2007 Article 9012Karen PinemNo ratings yet
- Table 1. Cardiotrophin-1: Characteristic Group LVH (N 45) Non LVH (N 30)Document2 pagesTable 1. Cardiotrophin-1: Characteristic Group LVH (N 45) Non LVH (N 30)Karen PinemNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Zoo Design ThesisDocument8 pagesZoo Design Thesistsivhqvcf100% (2)
- 8 - Properties - of - Communication PURCOMM LESSON1Document4 pages8 - Properties - of - Communication PURCOMM LESSON1Jerico PitaNo ratings yet
- Coal Combustion (Zlibraryexau2g3p.onion)Document247 pagesCoal Combustion (Zlibraryexau2g3p.onion)Ardita S IrwanNo ratings yet
- Ecw331 Chapter 05 Final PDFDocument37 pagesEcw331 Chapter 05 Final PDFMuhd MuqhreyNo ratings yet
- الاوكسجين المذاب PDFDocument67 pagesالاوكسجين المذاب PDFMajeed Al AnbarieyNo ratings yet
- Positive Psychology: A HandbookDocument48 pagesPositive Psychology: A HandbookSuVam LeoChanNo ratings yet
- The Substantial DerivativeDocument1 pageThe Substantial DerivativeNielNo ratings yet
- Enrichment material for the 12th grade -استردادDocument13 pagesEnrichment material for the 12th grade -استردادnananaimNo ratings yet
- Development of Risk Trageted Ground Motions Asce7Document33 pagesDevelopment of Risk Trageted Ground Motions Asce7Khalid WaziraNo ratings yet
- Anthropology and The Changing WorldDocument12 pagesAnthropology and The Changing Worldbilal1710No ratings yet
- TNPCB PDFDocument231 pagesTNPCB PDFGunaseelan RvNo ratings yet
- Gaucher's DiseaseDocument26 pagesGaucher's DiseasealxxndraromeroNo ratings yet
- Linear Equations in One VariableDocument10 pagesLinear Equations in One VariableRiddhiman BoseNo ratings yet
- Pajarillo, Villanada&Ruedas - Food SafetyDocument13 pagesPajarillo, Villanada&Ruedas - Food SafetyMary Yole Apple DeclaroNo ratings yet
- Etsa V3Document18 pagesEtsa V3Robbani HamdanNo ratings yet
- DLSZ BRafeNHS Recommendation Form AY 2023 2024Document2 pagesDLSZ BRafeNHS Recommendation Form AY 2023 2024KrskieNo ratings yet
- Ucsp Module 6 W:B Answer SheetDocument5 pagesUcsp Module 6 W:B Answer SheetAl Cheeno Anonuevo100% (1)
- 7 Gastroenteritis Nursing Care Plans - NurseslabsDocument8 pages7 Gastroenteritis Nursing Care Plans - NurseslabsHikaru Takishima91% (23)
- Feminist Essay TopicsDocument6 pagesFeminist Essay Topicsxsfazwwhd100% (2)
- Extended Report On Weld Joint TestingDocument44 pagesExtended Report On Weld Joint TestingRajbanul AkhondNo ratings yet
- An Investigation On Gas Lift Performance Curve in An Oil Producing Well (Deni Saepudin)Document16 pagesAn Investigation On Gas Lift Performance Curve in An Oil Producing Well (Deni Saepudin)Atrian RahadiNo ratings yet
- Giorgi-2003-Descriptive Phenomenological Psychological Method PDFDocument31 pagesGiorgi-2003-Descriptive Phenomenological Psychological Method PDFAngie Paola Monsalve RuizNo ratings yet
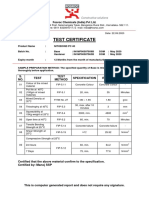
- Test Certificate: S. NO. Test Test Method Specification Result UOMDocument1 pageTest Certificate: S. NO. Test Test Method Specification Result UOMkaushik100% (1)
- Ta840 Tg-L1019eDocument5 pagesTa840 Tg-L1019eKaleem KhanNo ratings yet
- Ice Slurry Applications PDFDocument15 pagesIce Slurry Applications PDFmattiturboNo ratings yet
- Total Selected ListDocument32 pagesTotal Selected ListVamsi KrishnaNo ratings yet
- Acf AppliedDocument2 pagesAcf AppliedBhargava Kumar Sompalli BoyaNo ratings yet
- Mycological Contributions of Rolf SingerDocument144 pagesMycological Contributions of Rolf SingerAmaterasuNo ratings yet
- Grade 9 English FAL SummariesDocument7 pagesGrade 9 English FAL SummariesEliciaNo ratings yet
- Strength Based Student ProfileDocument1 pageStrength Based Student Profileapi-544895801No ratings yet