You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pilot Exam 2020Document5 pagesPilot Exam 2020Nikita AtrahimovicsNo ratings yet
- 13 Methods of Identification in Forensic Medicine1Document36 pages13 Methods of Identification in Forensic Medicine1TiaRa JuraidNo ratings yet
- 13 Profesionalism and Managerial SkillDocument16 pages13 Profesionalism and Managerial SkillTiaRa JuraidNo ratings yet
- 13 Profesionalism and Managerial SkillDocument16 pages13 Profesionalism and Managerial SkillTiaRa JuraidNo ratings yet
- 13 Profesionalism and Managerial SkillDocument16 pages13 Profesionalism and Managerial SkillTiaRa JuraidNo ratings yet
- 12 Health PolicyDocument18 pages12 Health PolicyTiaRa JuraidNo ratings yet
- 11 Kesehatan MasyarakatDocument48 pages11 Kesehatan MasyarakatTiaRa JuraidNo ratings yet
- 12 Health PolicyDocument18 pages12 Health PolicyTiaRa JuraidNo ratings yet
- 11 Kesehatan MasyarakatDocument48 pages11 Kesehatan MasyarakatTiaRa JuraidNo ratings yet
- Translate Part 1Document22 pagesTranslate Part 1TiaRa JuraidNo ratings yet
- Ormood Aits ,: Tory Failure Reaso, As For Which May Be The Primary ReasonDocument6 pagesOrmood Aits ,: Tory Failure Reaso, As For Which May Be The Primary ReasonTiaRa JuraidNo ratings yet
- Xenobiotics 2015Document52 pagesXenobiotics 2015TiaRa JuraidNo ratings yet
- Ormood Aits ,: Tory Failure Reaso, As For Which May Be The Primary ReasonDocument6 pagesOrmood Aits ,: Tory Failure Reaso, As For Which May Be The Primary ReasonTiaRa JuraidNo ratings yet
- Department of Histology and Cell Biology Faculty of Medicine Universitas Gadjah MadaDocument14 pagesDepartment of Histology and Cell Biology Faculty of Medicine Universitas Gadjah MadaTiaRa JuraidNo ratings yet
- Acid Base EquilibriumDocument43 pagesAcid Base EquilibriumNi Made Dwiki AndriyaniNo ratings yet
- Metabolic Rate Dan BMR: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMDocument78 pagesMetabolic Rate Dan BMR: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMTiaRa JuraidNo ratings yet
- Jadwal Blok 9 Untad 2016 Rev 25012016Document7 pagesJadwal Blok 9 Untad 2016 Rev 25012016TiaRa JuraidNo ratings yet
- Metabolic Rate Dan BMR: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMDocument78 pagesMetabolic Rate Dan BMR: DR - Dr.zaenal M. Sofro, AIFM, Sport & Circ. Med. Bagian Ilmu Faal Fak - Kedokteran UGMTiaRa JuraidNo ratings yet
- 13 Evidence Based Medicine 2014Document17 pages13 Evidence Based Medicine 2014TiaRa JuraidNo ratings yet
- 16 English in MedicineDocument15 pages16 English in MedicineTiaRa JuraidNo ratings yet
- 4 Elderly Fractures Tidak Di BahasDocument35 pages4 Elderly Fractures Tidak Di BahasTiaRa JuraidNo ratings yet
- Musculoskeletal SystemDocument76 pagesMusculoskeletal SystemTiaRa JuraidNo ratings yet
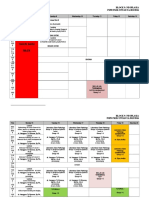
- Block 10: Musculoskeletal and Locomotion PSPD FKIK UNTAD TA. 2015/2016 WEEK 1: 28 Maret - 2 April 2016Document7 pagesBlock 10: Musculoskeletal and Locomotion PSPD FKIK UNTAD TA. 2015/2016 WEEK 1: 28 Maret - 2 April 2016TiaRa JuraidNo ratings yet
- LO Blok 22 Skenario 3Document5 pagesLO Blok 22 Skenario 3TiaRa JuraidNo ratings yet
- BMC Med EducDocument12 pagesBMC Med EducTiaRa JuraidNo ratings yet
- 7.1 Sources and Forms of Energy Learning Standard: Pupils Are Able ToDocument5 pages7.1 Sources and Forms of Energy Learning Standard: Pupils Are Able ToZulkifly Md AlwayiNo ratings yet
- IAReceipt Acknowledgement FormDocument1 pageIAReceipt Acknowledgement FormYogita NaikNo ratings yet
- Law Case Study AnalysisDocument3 pagesLaw Case Study Analysisapi-323713948No ratings yet
- Jack Welch: Navigation SearchDocument12 pagesJack Welch: Navigation SearchGordanaMrđaNo ratings yet
- VSICM55 M01 CourseIntro PDFDocument12 pagesVSICM55 M01 CourseIntro PDFandyNo ratings yet
- DLP in Filipino For Observation RevisedDocument4 pagesDLP in Filipino For Observation RevisedLissa Mae Macapobre100% (1)
- Kenedy G. Flores (June 2021)Document2 pagesKenedy G. Flores (June 2021)KENEDY FLORESNo ratings yet
- Chapter 3Document23 pagesChapter 3Shahmeer AliNo ratings yet
- George Washington UniversityDocument8 pagesGeorge Washington UniversityMichaelNo ratings yet
- Kvs Accounts Code LatestDocument299 pagesKvs Accounts Code LatestManju ChahalNo ratings yet
- Technical Writing Course Manual, Spring 2021Document34 pagesTechnical Writing Course Manual, Spring 2021rajdharmkarNo ratings yet
- Unit IV. Communication in Pharmacy Practice PDFDocument54 pagesUnit IV. Communication in Pharmacy Practice PDFGeannea Mae LeañoNo ratings yet
- Math 7 q4 Module 4 and 5 - Using Appropriate Graphs To Represent Organized Data - Dfdjnhs NewDocument23 pagesMath 7 q4 Module 4 and 5 - Using Appropriate Graphs To Represent Organized Data - Dfdjnhs NewJen TarioNo ratings yet
- Lopena RPH Page 1 25 ReviewerDocument2 pagesLopena RPH Page 1 25 ReviewerchingchongNo ratings yet
- The Cincinnati Enquirer March: Chester Nettrower CollectionDocument21 pagesThe Cincinnati Enquirer March: Chester Nettrower Collectioncreeva2912No ratings yet
- NIA 1 - National Investigation Agency - Deputaion Nomination - DT 07.09.21Document10 pagesNIA 1 - National Investigation Agency - Deputaion Nomination - DT 07.09.21Adarsh DixitNo ratings yet
- CSS Forums - View Single Post - PMS SyllabusDocument9 pagesCSS Forums - View Single Post - PMS SyllabusAdnan AbbasNo ratings yet
- Sexing The CherryDocument8 pagesSexing The CherryAndreea Cristina Funariu100% (1)
- Job Description Associate Attorney 2019Document5 pagesJob Description Associate Attorney 2019SAI SUVEDHYA RNo ratings yet
- Aires DLP English 10Document6 pagesAires DLP English 10Aljean Taylaran AsbiNo ratings yet
- TO Questioned Documents: Darwin P. Batawang, Ph.D. CrimDocument54 pagesTO Questioned Documents: Darwin P. Batawang, Ph.D. Crimako si XianNo ratings yet
- International Baccalaureate ProgrammeDocument5 pagesInternational Baccalaureate Programmeapi-280508830No ratings yet
- Week 1 The Scientific Method of ResearchDocument12 pagesWeek 1 The Scientific Method of ResearchJia Jun VooNo ratings yet
- PAPERS #10 EnglishDocument21 pagesPAPERS #10 EnglishdozegrzaNo ratings yet
- School To Club Sport Transition: Strategy and Product Design EssentialsDocument8 pagesSchool To Club Sport Transition: Strategy and Product Design EssentialsSamuel AyelignNo ratings yet
- National Gallery Singapore ReflectionsDocument4 pagesNational Gallery Singapore Reflectionsverna_goh_shileiNo ratings yet
- 12 Statistics and Probability G11 Quarter 4 Module 12 Computating For The Test Statistic Involving Population ProportionDocument27 pages12 Statistics and Probability G11 Quarter 4 Module 12 Computating For The Test Statistic Involving Population ProportionLerwin Garinga100% (9)
- Présentation Bootcamp 1 orDocument31 pagesPrésentation Bootcamp 1 orwalid laqrafiNo ratings yet
- Games and Economic Behavior Volume 14 Issue 2 1996 (Doi 10.1006/game.1996.0053) Roger B. Myerson - John Nash's Contribution To Economics PDFDocument9 pagesGames and Economic Behavior Volume 14 Issue 2 1996 (Doi 10.1006/game.1996.0053) Roger B. Myerson - John Nash's Contribution To Economics PDFEugenio MartinezNo ratings yet