You might also like
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- Family Medicine Family CaseDocument17 pagesFamily Medicine Family Casecorina_oliverNo ratings yet
- Family CEADocument3 pagesFamily CEAnge257100% (1)
- EpdsDocument2 pagesEpdsapi-254209971No ratings yet
- Personal Entrepreneurial Competencies PECG8 9Document16 pagesPersonal Entrepreneurial Competencies PECG8 9maria nia ferueloNo ratings yet
- Angelina Alphonce JohoDocument80 pagesAngelina Alphonce JohoMerlina WijayawatiNo ratings yet
- Types of EntreprenursDocument2 pagesTypes of EntreprenursValar Morghulis100% (2)
- Prevention and Control of Infection MissionDocument8 pagesPrevention and Control of Infection MissionYana OrtegaNo ratings yet
- FCM1 - S01-T01-Introduction To FCM and The Five Star Doctor PDFDocument6 pagesFCM1 - S01-T01-Introduction To FCM and The Five Star Doctor PDFGianne OgacoNo ratings yet
- Care of The Elderly: Presented By: Roselily CoquillaDocument33 pagesCare of The Elderly: Presented By: Roselily CoquillaOng KarlNo ratings yet
- Geriatric Nurses Care For The ElderlyDocument4 pagesGeriatric Nurses Care For The ElderlyIconMaicoNo ratings yet
- Cga - 1Document19 pagesCga - 1Kenji Tolero100% (1)
- Periodic Health ExamDocument23 pagesPeriodic Health ExamPernel Jose Alam MicuboNo ratings yet
- Philippine College of Health Science IncDocument23 pagesPhilippine College of Health Science Incpeter bruceNo ratings yet
- Aims and Objective of Expanded Program of ImmunizationDocument18 pagesAims and Objective of Expanded Program of Immunizationpaperpin27100% (2)
- TB in ChildrenDocument26 pagesTB in ChildrenReagan PatriarcaNo ratings yet
- 05 Headss PDFDocument2 pages05 Headss PDFКонстантин КрахмалевNo ratings yet
- Comprehensive School Health AssessmentDocument8 pagesComprehensive School Health Assessmentapi-308397176No ratings yet
- The 4 Box Method - Practical ApproachDocument39 pagesThe 4 Box Method - Practical ApproachramwshNo ratings yet
- Impact of IllnessDocument53 pagesImpact of IllnessDitas ChuNo ratings yet
- Hypertension Protocol JeannineDocument53 pagesHypertension Protocol JeannineAleile DRNo ratings yet
- Benefit Packages For Inpatient Care of Probable and Confirmed COVID-19 Developing Severe Illness / OutcomesDocument31 pagesBenefit Packages For Inpatient Care of Probable and Confirmed COVID-19 Developing Severe Illness / OutcomesGeneXpert Lab LCPNo ratings yet
- Updated Guidelines on Management of Animal Bite PatientsDocument15 pagesUpdated Guidelines on Management of Animal Bite PatientsKaren ArchesNo ratings yet
- Filipino Concepts of Health, Illness and DiseaseDocument43 pagesFilipino Concepts of Health, Illness and DiseaseFelisa Lacsamana Gregorio50% (2)
- Patient's RightsDocument7 pagesPatient's RightsLorraine RiegoNo ratings yet
- HAB ManualDocument102 pagesHAB ManualSven OrdanzaNo ratings yet
- Reading Comprehension: 1. Are The Following Statements True or False ? Justify!Document2 pagesReading Comprehension: 1. Are The Following Statements True or False ? Justify!anaNo ratings yet
- SOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticDocument5 pagesSOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticvidyahamzahNo ratings yet
- Chapter 4 (Malpractice)Document5 pagesChapter 4 (Malpractice)Maan QuilangNo ratings yet
- Congenital Rubella SyndromeDocument8 pagesCongenital Rubella SyndromeIman HendriantoNo ratings yet
- Pros and Cons of Abortion DebateDocument3 pagesPros and Cons of Abortion DebateHeru PamitanMinggatt AssalamualaikumNo ratings yet
- Managing Head Injuries: Medical and Surgical ApproachesDocument38 pagesManaging Head Injuries: Medical and Surgical ApproachesAmanuel AyladoNo ratings yet
- SCREEM (Divina) resources pathology planDocument2 pagesSCREEM (Divina) resources pathology planDranreb Berylle MasangkayNo ratings yet
- Grupo 10 Non-Technical Skills in HistopathologyDocument9 pagesGrupo 10 Non-Technical Skills in HistopathologySantos Pardo Gomez100% (1)
- Primary Health Care Maternal & Child HealthDocument32 pagesPrimary Health Care Maternal & Child HealthAbidah Rahmi HilmyNo ratings yet
- Ethical Issues in HIV ConfidentialityDocument12 pagesEthical Issues in HIV ConfidentialityVinia A. VillanuevaNo ratings yet
- Family Health NursingDocument17 pagesFamily Health NursingMIKAELLA BALUNANNo ratings yet
- PAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFDocument35 pagesPAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFZaqueo Gutierrez FajardoNo ratings yet
- Impact of Illness on FamilyDocument29 pagesImpact of Illness on FamilyMuhammad Gilang DwiputraNo ratings yet
- Child Health Strategic Plan 2001-2004Document26 pagesChild Health Strategic Plan 2001-2004Sai BondadNo ratings yet
- And The Band Played OnDocument2 pagesAnd The Band Played OnRider NoaNo ratings yet
- PHC 1 ModuleDocument136 pagesPHC 1 ModuleRoselyn MadiwoNo ratings yet
- Patients RightsDocument15 pagesPatients RightsJulie Ann Marie Dalisay-UyNo ratings yet
- Key Steps of Evidence-Based Practice: What Type of Question Are You Asking and What Will The Evidence Support?Document29 pagesKey Steps of Evidence-Based Practice: What Type of Question Are You Asking and What Will The Evidence Support?Ron OpulenciaNo ratings yet
- Medical Malpractice Case AnalysisDocument20 pagesMedical Malpractice Case AnalysisMJ CarreonNo ratings yet
- PowerPoint on Infectious DiseasesDocument24 pagesPowerPoint on Infectious DiseasesgabmusaNo ratings yet
- Obstetric HistoryDocument38 pagesObstetric HistoryHannah LeianNo ratings yet
- 1980 - Smilkstein's Cycle of Family FunctionDocument9 pages1980 - Smilkstein's Cycle of Family FunctionJoshua Benjamin Rocamora GrapaNo ratings yet
- An Introduction To Evidence-Based NursinDocument8 pagesAn Introduction To Evidence-Based NursinAli MaqsudiNo ratings yet
- DOH DM 2019 0062 HepB Demo Project With Interim GuidelinesDocument31 pagesDOH DM 2019 0062 HepB Demo Project With Interim GuidelinesRold Brio SosNo ratings yet
- EpendymomaDocument5 pagesEpendymomaDenny's BerciaNo ratings yet
- Ethics in PediatricsDocument20 pagesEthics in PediatricsCruz YrNo ratings yet
- Strategies To Deal With Uncertainty in Medicine 20Document2 pagesStrategies To Deal With Uncertainty in Medicine 20Emilio AssisNo ratings yet
- Cruz BG 1Document408 pagesCruz BG 1kimNo ratings yet
- Concepts of Health and IllnessDocument4 pagesConcepts of Health and IllnessDes SayNo ratings yet
- An Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CareDocument18 pagesAn Integrative Literature Review On Post Organ Transplant Mortality Due To Renal Failure: Causes and Nursing CarePATRICK OTIATONo ratings yet
- CPM18th Care of Older PersonsDocument11 pagesCPM18th Care of Older PersonsWila GatchalianNo ratings yet
- PDS 2014 Annual Report PDFDocument18 pagesPDS 2014 Annual Report PDFdoctorkwekkwekNo ratings yet
- MedicoLegalConsensus - 3.10 Ver 2Document116 pagesMedicoLegalConsensus - 3.10 Ver 2Alqueen AlmonteNo ratings yet
- CPG AbortionDocument40 pagesCPG AbortionGina Margaret BallesterosNo ratings yet
- Chemoman - TwoDocument1 pageChemoman - TwoJoan LuisNo ratings yet
- Chemo ManDocument1 pageChemo ManJoan LuisNo ratings yet
- Proper cough and sneeze etiquetteDocument3 pagesProper cough and sneeze etiquetteJoan LuisNo ratings yet
- Acute Kidney Injury in ChildDocument6 pagesAcute Kidney Injury in ChildJoan LuisNo ratings yet
- Family AssessmentDocument10 pagesFamily AssessmentJoan LuisNo ratings yet
- Nutrition Natalie C. Maramba, M.DDocument4 pagesNutrition Natalie C. Maramba, M.DJoan LuisNo ratings yet
- Family Life Cycle: Berguia, Bryan - Luis, Joan - Maramba, Natalie - Untalan, NatashaDocument6 pagesFamily Life Cycle: Berguia, Bryan - Luis, Joan - Maramba, Natalie - Untalan, NatashaJoan LuisNo ratings yet
- TB AdenitisDocument7 pagesTB AdenitisJoan LuisNo ratings yet
- CPG On Acute GastroenteritisDocument24 pagesCPG On Acute GastroenteritisJoan LuisNo ratings yet
- CPG On Acute GastroenteritisDocument24 pagesCPG On Acute GastroenteritisJoan LuisNo ratings yet
- Acute Respiratory Infections Daryl Joel Dumdum, M.DDocument5 pagesAcute Respiratory Infections Daryl Joel Dumdum, M.DJoan LuisNo ratings yet
- CARE Checklist (2013) of Information To Include When Writing A Case ReportDocument1 pageCARE Checklist (2013) of Information To Include When Writing A Case ReportJoan LuisNo ratings yet
- SmokingDocument2 pagesSmokingJoan LuisNo ratings yet
- Teen Pregnancy and STI RisksDocument23 pagesTeen Pregnancy and STI RisksJoan LuisNo ratings yet
- Metrics: Disability-Adjusted Life Year (DALY) : Social Value Weights (Age-Weighting and Discounting)Document1 pageMetrics: Disability-Adjusted Life Year (DALY) : Social Value Weights (Age-Weighting and Discounting)Joan LuisNo ratings yet
- Sis TrunkDocument1 pageSis TrunkJoan LuisNo ratings yet
- Article 06Document6 pagesArticle 06Mega MuzdalifahNo ratings yet
- Cardio MnemonicsDocument5 pagesCardio MnemonicsJoan LuisNo ratings yet
- 5 PlasmodiaDocument99 pages5 PlasmodiaJoan LuisNo ratings yet
- Accomplishment List Accomplishment List: (Topics I Have Read) (Topics I Have Read)Document1 pageAccomplishment List Accomplishment List: (Topics I Have Read) (Topics I Have Read)Joan LuisNo ratings yet
- Pediatric Case PresentationDocument71 pagesPediatric Case PresentationJoan Luis100% (1)
- Thoracic Aortic Aneurysm & Dissection PDFDocument140 pagesThoracic Aortic Aneurysm & Dissection PDFJoan LuisNo ratings yet
- Surgical Management of Peptic Ulcer Disease ComplicationsDocument57 pagesSurgical Management of Peptic Ulcer Disease ComplicationsJoan LuisNo ratings yet
- CPM7th TB in Infancy and ChildhoodDocument41 pagesCPM7th TB in Infancy and ChildhoodJackyNo ratings yet
- IMCI Chart Booklet PDFDocument80 pagesIMCI Chart Booklet PDFmikay100% (1)
- Leptospirosis CPG 2010 PDFDocument66 pagesLeptospirosis CPG 2010 PDFRogelio Junior RiveraNo ratings yet
- Accomplishment List Accomplishment List: (Topics I Have Read) (Topics I Have Read)Document1 pageAccomplishment List Accomplishment List: (Topics I Have Read) (Topics I Have Read)Joan LuisNo ratings yet
- Obstetric Anatomy: Professor of Obstetrics & Gynecology Ain Shams Faculty of MedicineDocument67 pagesObstetric Anatomy: Professor of Obstetrics & Gynecology Ain Shams Faculty of MedicineJoan LuisNo ratings yet
- H. Pylori eradication and PPI treatment for peptic ulcer diseaseDocument9 pagesH. Pylori eradication and PPI treatment for peptic ulcer diseaseJoan LuisNo ratings yet
- CPG-Coronary Artery Disease (2014)Document120 pagesCPG-Coronary Artery Disease (2014)lovelots1234No ratings yet
- The Legend - Larry Scott Workout and Diet Iron & GritDocument15 pagesThe Legend - Larry Scott Workout and Diet Iron & GritAtharva100% (3)
- Positive Step Towards A Unsatisfied, Depressed Life With Laventrix Shilajit CapsulesDocument3 pagesPositive Step Towards A Unsatisfied, Depressed Life With Laventrix Shilajit CapsulesNicole Nikka Mike ClarenceNo ratings yet
- Multivitamin Ebook Updated Sept 2023Document30 pagesMultivitamin Ebook Updated Sept 2023szleaNo ratings yet
- Dabur India LimitedDocument6 pagesDabur India LimitedJammigumpula PriyankaNo ratings yet
- Nutritional Recommendations For Physique AthletesDocument30 pagesNutritional Recommendations For Physique AthletesAngie CarolineNo ratings yet
- CH 11Document28 pagesCH 11api-254748913No ratings yet
- Annex 3 WHO TRS 1011 Web-7Document121 pagesAnnex 3 WHO TRS 1011 Web-7Jaime Andrés García BNo ratings yet
- Vitamin D & Alopecia AreataDocument2 pagesVitamin D & Alopecia AreataMohitNo ratings yet
- Herbalife Product Brochure 2018Document33 pagesHerbalife Product Brochure 2018maxNo ratings yet
- Malnutrition in Older Adults: An Evidence-Based Review of Risk Factors, Assessment, and InterventionDocument8 pagesMalnutrition in Older Adults: An Evidence-Based Review of Risk Factors, Assessment, and InterventionDago DagoNo ratings yet
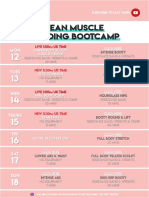
- 26 - LEAN Weekly Guide - On - October 12Document15 pages26 - LEAN Weekly Guide - On - October 12Andrea CsillaNo ratings yet
- Vitamin B10 (PABA) - Uses, Safety, and DosageDocument11 pagesVitamin B10 (PABA) - Uses, Safety, and DosageAri Sa FaNo ratings yet
- Limiting Feed Intake With Salt Afs 3008Document2 pagesLimiting Feed Intake With Salt Afs 3008Frederico Velasco - Ruminantes (São Paulo)No ratings yet
- NUTR 207 FA14 SyllabusDocument2 pagesNUTR 207 FA14 SyllabusninahemesNo ratings yet
- Dandelion Root (Taraxacum Officinale) Herbal Monograph - Brett ElliottDocument8 pagesDandelion Root (Taraxacum Officinale) Herbal Monograph - Brett Elliottboob bobsonnnNo ratings yet
- Method For The Determination of Beta Carotene in Supplements and Raw Materials by Reversed Phase Liquid Chromatography Single Laboratory ValidationDocument13 pagesMethod For The Determination of Beta Carotene in Supplements and Raw Materials by Reversed Phase Liquid Chromatography Single Laboratory ValidationChris JohnsonNo ratings yet
- Malnutrisi Energi Protein: Dr. Mars Nashrah A, M.Ked (Ped), SpaDocument88 pagesMalnutrisi Energi Protein: Dr. Mars Nashrah A, M.Ked (Ped), SpaDiana NusantariNo ratings yet
- DrFormulas® To Offer Black Friday and Cyber Monday Deals in NovemberDocument2 pagesDrFormulas® To Offer Black Friday and Cyber Monday Deals in NovemberPR.comNo ratings yet
- Better NutritionDocument60 pagesBetter NutritionSoni Gupta100% (1)
- Are We Making The Most of SupplementsDocument3 pagesAre We Making The Most of SupplementsEmmanuel SánchezNo ratings yet
- Project Proposal - BSMA 1202 byDocument19 pagesProject Proposal - BSMA 1202 byFabbi FababairNo ratings yet
- Family Formula NestleDocument25 pagesFamily Formula NestleDavid LeeNo ratings yet
- AGQ Cliff NotesDocument42 pagesAGQ Cliff NotesMitchellFelixNo ratings yet
- Nutraceutical - Definition and Introduction - Kalra2003 PDFDocument2 pagesNutraceutical - Definition and Introduction - Kalra2003 PDFjoseNo ratings yet
- Foreword: Food Services ManualDocument650 pagesForeword: Food Services ManualmableyNo ratings yet
- Internship Report (LIN)Document18 pagesInternship Report (LIN)aditya patelNo ratings yet
- Chemical Adulterants in Herbal Medicinal Products: A Review: Authors AffiliationsDocument11 pagesChemical Adulterants in Herbal Medicinal Products: A Review: Authors AffiliationseyobNo ratings yet
- Gary Null - The Complete Encyclopedia of Natural Healing - Gary NullDocument520 pagesGary Null - The Complete Encyclopedia of Natural Healing - Gary NullEbook PDF100% (7)
- Special Program in Sports Curriculum MapDocument10 pagesSpecial Program in Sports Curriculum MapDiane MaryNo ratings yet
- A-MIDTERMS EXAM-NutriLEC - To PrintDocument9 pagesA-MIDTERMS EXAM-NutriLEC - To PrintNelia AlfonsoNo ratings yet
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusFrom EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusRating: 4.5 out of 5 stars4.5/5 (10)
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (5)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeFrom EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNo ratings yet
- Epidemics and Society: From the Black Death to the PresentFrom EverandEpidemics and Society: From the Black Death to the PresentRating: 4.5 out of 5 stars4.5/5 (9)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyRating: 4 out of 5 stars4/5 (18)
- The HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedFrom EverandThe HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedRating: 4.5 out of 5 stars4.5/5 (13)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryFrom EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryRating: 4 out of 5 stars4/5 (6)
- Quick Fixes: Drugs in America from Prohibition to the 21st Century BingeFrom EverandQuick Fixes: Drugs in America from Prohibition to the 21st Century BingeNo ratings yet
- The Transformation: Discovering Wholeness and Healing After TraumaFrom EverandThe Transformation: Discovering Wholeness and Healing After TraumaRating: 4 out of 5 stars4/5 (70)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- Microbiological Quality of FoodsFrom EverandMicrobiological Quality of FoodsL SlanetzNo ratings yet
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthFrom EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo ratings yet
- Blood Runs Coal: The Yablonski Murders and the Battle for the United Mine Workers of AmericaFrom EverandBlood Runs Coal: The Yablonski Murders and the Battle for the United Mine Workers of AmericaRating: 4.5 out of 5 stars4.5/5 (2)
- A Good Time to Be Born: How Science and Public Health Gave Children a FutureFrom EverandA Good Time to Be Born: How Science and Public Health Gave Children a FutureRating: 5 out of 5 stars5/5 (1)
- The War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical BoardFrom EverandThe War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical BoardRating: 3 out of 5 stars3/5 (2)
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefFrom EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNo ratings yet
- War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicFrom EverandWar on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicRating: 4 out of 5 stars4/5 (7)
- Doctored: The Disillusionment of an American PhysicianFrom EverandDoctored: The Disillusionment of an American PhysicianRating: 4 out of 5 stars4/5 (11)