You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 06 BuyLog2013 MoldedCaseCircBrkrsDocument106 pages06 BuyLog2013 MoldedCaseCircBrkrsmarbyNo ratings yet
- Chap 14Document31 pagesChap 14Dipti Bhavin DesaiNo ratings yet
- FinTech RegTech and SupTech - What They Mean For Financial Supervision FINALDocument19 pagesFinTech RegTech and SupTech - What They Mean For Financial Supervision FINALirvandi syahputraNo ratings yet
- FMDQ Codified Rule Book FGN BondsDocument65 pagesFMDQ Codified Rule Book FGN BondsOladipupo Mayowa PaulNo ratings yet
- Mysuru Royal Institute of Technology. Mandya: Question Bank-1Document2 pagesMysuru Royal Institute of Technology. Mandya: Question Bank-1chaitragowda213_4732No ratings yet
- Chapter 3 SampleDocument12 pagesChapter 3 Samplesyarifah53No ratings yet
- Summary Studying Public Policy Michael Howlett CompleteDocument28 pagesSummary Studying Public Policy Michael Howlett CompletefadwaNo ratings yet
- Refference 01 Sheethal Visa Rejection Reason ExplanationDocument3 pagesRefference 01 Sheethal Visa Rejection Reason ExplanationAniket PatelNo ratings yet
- 1.1 Cruz v. DENR PDFDocument7 pages1.1 Cruz v. DENR PDFBenBulacNo ratings yet
- Process Plant Layout and Piping DesignDocument4 pagesProcess Plant Layout and Piping Designktsnl100% (1)
- Dominar 400 Spare Parts CatalogueDocument82 pagesDominar 400 Spare Parts CatalogueAkshayaNo ratings yet
- ETA-1 Service PDFDocument44 pagesETA-1 Service PDFgansolNo ratings yet
- Odontogenic CystsDocument5 pagesOdontogenic CystsBH ASMRNo ratings yet
- Determination of Sales Force Size - 2Document2 pagesDetermination of Sales Force Size - 2Manish Kumar100% (3)
- SecureCore Datasheet V2Document2 pagesSecureCore Datasheet V2chepogaviriaf83No ratings yet
- Stps 20 H 100 CTDocument8 pagesStps 20 H 100 CTPablo Cruz ArchundiaNo ratings yet
- Roundup WG Bula MonsantoDocument16 pagesRoundup WG Bula MonsantodandanyddNo ratings yet
- HK Magazine 03082013Document56 pagesHK Magazine 03082013apparition9No ratings yet
- Tarlac - San Antonio - Business Permit - NewDocument2 pagesTarlac - San Antonio - Business Permit - Newarjhay llave100% (1)
- JKR SPJ 1988 Standard Specification of Road Works - Section 1 - GeneralDocument270 pagesJKR SPJ 1988 Standard Specification of Road Works - Section 1 - GeneralYamie Rozman100% (1)
- CS 148 - Introduction To Computer Graphics and ImagingDocument3 pagesCS 148 - Introduction To Computer Graphics and ImagingMurtaza TajNo ratings yet
- Splunk Certification: Certification Exam Study GuideDocument18 pagesSplunk Certification: Certification Exam Study GuidesalemselvaNo ratings yet
- Muhammad Safuan Othman (CD 4862)Document24 pagesMuhammad Safuan Othman (CD 4862)Andy100% (1)
- Occupational Stress Questionnaire PDFDocument5 pagesOccupational Stress Questionnaire PDFabbaskhodaei666No ratings yet
- High Performance Computing in Power System Applications.: September 1996Document24 pagesHigh Performance Computing in Power System Applications.: September 1996Ahmed adelNo ratings yet
- 3d Mug Tutorial in 3d MaxDocument5 pages3d Mug Tutorial in 3d MaxCalvin TejaNo ratings yet
- Media ReportDocument46 pagesMedia ReportAndrew AB BurgoonNo ratings yet
- Taller Sobre Preposiciones y Vocabulario - Exhibición Comercial SergioDocument5 pagesTaller Sobre Preposiciones y Vocabulario - Exhibición Comercial SergioYovanny Peña Pinzon100% (2)
- 3-Matic 14 - User Manual 15Document169 pages3-Matic 14 - User Manual 15Oliver RuizNo ratings yet
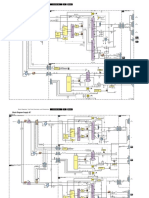
- Philips Chassis Lc4.31e Aa Power Dps 181 PDFDocument9 pagesPhilips Chassis Lc4.31e Aa Power Dps 181 PDFAouadi AbdellazizNo ratings yet