You might also like
- Fluorescence Microscopy: Super-Resolution and other Novel TechniquesFrom EverandFluorescence Microscopy: Super-Resolution and other Novel TechniquesAnda CorneaNo ratings yet
- Texture AnalysisDocument6 pagesTexture AnalysisSumit ChakravartyNo ratings yet
- 1 s2.0 S089579671730011X MainDocument10 pages1 s2.0 S089579671730011X MainquodicNo ratings yet
- Perbedaan Benigna Dan MalignaDocument7 pagesPerbedaan Benigna Dan MalignaEndang Rahayu Fuji LestaryNo ratings yet
- Baran Et Al-2016-Journal of BiophotonicsDocument9 pagesBaran Et Al-2016-Journal of BiophotonicsJuan DovalNo ratings yet
- IVUS Vs OCT For Mechanism and Patterns of In-Stent RestenosisDocument5 pagesIVUS Vs OCT For Mechanism and Patterns of In-Stent RestenosisDuchung TranNo ratings yet
- Cholesterol Crystals in Non-Culprit Plaques of STEMI Patients A 3-Vessel OCT StudyDocument7 pagesCholesterol Crystals in Non-Culprit Plaques of STEMI Patients A 3-Vessel OCT StudysunhaolanNo ratings yet
- Texture TMIDocument6 pagesTexture TMIAnonymous 6WeX00mx0No ratings yet
- 8.nagabhushana - Nagabhushanrm@Document5 pages8.nagabhushana - Nagabhushanrm@Ademar Alves TrindadeNo ratings yet
- Characterization of Visually Similar Diffuse Diseases From B-Scan Liver Images Using Nonseparable Wavelet TransformDocument9 pagesCharacterization of Visually Similar Diffuse Diseases From B-Scan Liver Images Using Nonseparable Wavelet TransformMuhammad WaqasNo ratings yet
- Diagnosis of Atherosclerosis by Imaging. - AJM.2008Document11 pagesDiagnosis of Atherosclerosis by Imaging. - AJM.2008Carlos MurilloNo ratings yet
- Comparing CVA Defects To Local RNFLDocument9 pagesComparing CVA Defects To Local RNFLkagone walidNo ratings yet
- I1552 5783 57 9 Oct51Document18 pagesI1552 5783 57 9 Oct51Vladimir KobelevNo ratings yet
- Low Reliability of CBCT for Diagnosing TMJ Soft Tissue CalcificationDocument5 pagesLow Reliability of CBCT for Diagnosing TMJ Soft Tissue CalcificationMarinaNo ratings yet
- Radu. in Search For VP - Time To Rethink Current Concepts. EHJ 2011Document4 pagesRadu. in Search For VP - Time To Rethink Current Concepts. EHJ 2011Maria CardioNo ratings yet
- 1 s2.0 S2212440312000442 MainDocument6 pages1 s2.0 S2212440312000442 MainMarinaNo ratings yet
- CBCT of TMDDocument13 pagesCBCT of TMDzaidNo ratings yet
- Echo 5Document18 pagesEcho 5Indera VyasNo ratings yet
- Temporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTDocument6 pagesTemporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTNovi DwiyantiNo ratings yet
- Primary Clinical Study of Radiomics For Diagnosing Simple Bone Cyst of The JawDocument8 pagesPrimary Clinical Study of Radiomics For Diagnosing Simple Bone Cyst of The JawRodolpho VilelaNo ratings yet
- Optical Coherence Tomography: An Emerging Technology For Biomedical Imaging and Optical BiopsyDocument17 pagesOptical Coherence Tomography: An Emerging Technology For Biomedical Imaging and Optical BiopsyoverkindNo ratings yet
- THE 19th CONGRESS OF THE ROMANIAN SOCIETY OF ANATOMY - v4 PDFDocument241 pagesTHE 19th CONGRESS OF THE ROMANIAN SOCIETY OF ANATOMY - v4 PDFGeorgiana ZahariaNo ratings yet
- 2020 Mielotc PDFDocument15 pages2020 Mielotc PDFR M MNo ratings yet
- Evaluation of Maxillary Sinus Dimensions in GenderDocument8 pagesEvaluation of Maxillary Sinus Dimensions in Gendersignacc362No ratings yet
- Heterogeneous tissue characterization using ultrasound fractal analysis modelsDocument31 pagesHeterogeneous tissue characterization using ultrasound fractal analysis modelsBEKALUNo ratings yet
- Features of the choriocapillaris on four OCTA devicesDocument9 pagesFeatures of the choriocapillaris on four OCTA devicesWindy HapsariNo ratings yet
- Assessment of central cartilaginous tumor of the appendicular bone: inter-observer and intermodality agreement and comparison of diagnostic performance of CT and MRIDocument11 pagesAssessment of central cartilaginous tumor of the appendicular bone: inter-observer and intermodality agreement and comparison of diagnostic performance of CT and MRIsilvana mendoncaNo ratings yet
- Chapter 5: Radiological Anatomy: General AspectsDocument7 pagesChapter 5: Radiological Anatomy: General AspectsYel YuriNo ratings yet
- A New Method of MRI Examination For The Sternoclavicular JointsDocument12 pagesA New Method of MRI Examination For The Sternoclavicular JointsRafael CamposNo ratings yet
- LN3Document6 pagesLN3Haseeb QuadriNo ratings yet
- Contrast-Enhanced Ultrasonography of Hepatocellular Carcinoma: Correlation Between Quantitative Parameters and Histological GradingDocument9 pagesContrast-Enhanced Ultrasonography of Hepatocellular Carcinoma: Correlation Between Quantitative Parameters and Histological GradingUp TayyuNo ratings yet
- Araki Oct Nrc2022Document20 pagesAraki Oct Nrc2022leidyalexserraoNo ratings yet
- Fractal Analysis Differentiation of Nuclear and Vascular Patterns in Hepatocellular Carcinomas and Hepatic MetastasisDocument10 pagesFractal Analysis Differentiation of Nuclear and Vascular Patterns in Hepatocellular Carcinomas and Hepatic MetastasisGabriel IonescuNo ratings yet
- Vinay 1 PDFDocument15 pagesVinay 1 PDFHOD CSENo ratings yet
- Octa Birdshot Fawzi PaperDocument8 pagesOcta Birdshot Fawzi PaperPriyanka DocNo ratings yet
- Computers in Biology and Medicine: B. Nayebifar, H. Abrishami MoghaddamDocument8 pagesComputers in Biology and Medicine: B. Nayebifar, H. Abrishami MoghaddamMohammad RofiiNo ratings yet
- Iranjradiol 10 140Document8 pagesIranjradiol 10 140Orange PeachNo ratings yet
- AJNR - Reduction of Coil Mass Artifacts in High-REsolution Flat Detector Conebeam CT of Cerebral Stent-Assisted CoilingDocument9 pagesAJNR - Reduction of Coil Mass Artifacts in High-REsolution Flat Detector Conebeam CT of Cerebral Stent-Assisted CoilinglmcgarethNo ratings yet
- Guo 2013Document6 pagesGuo 2013OctavioJose DuarteFrenkyNo ratings yet
- Imaging in Osteoarthritis (2017) 2Document18 pagesImaging in Osteoarthritis (2017) 2Luis Nicolas Leon SuarezNo ratings yet
- MRI-Based Attenuation Correction For PET/MRI Using Ultrashort Echo Time SequencesDocument8 pagesMRI-Based Attenuation Correction For PET/MRI Using Ultrashort Echo Time SequencesOmarah AbdalqaderNo ratings yet
- Imaging For Neuro-Ophthalmic and Orbital Disease - A ReviewDocument24 pagesImaging For Neuro-Ophthalmic and Orbital Disease - A ReviewMashhoor AlfayezNo ratings yet
- At TomograpyhDocument9 pagesAt TomograpyhCarmen BaezNo ratings yet
- Radiol 2301030837Document2 pagesRadiol 2301030837john digiacomaNo ratings yet
- Endoscopic OCT With Forward-Looking Prob PDFDocument15 pagesEndoscopic OCT With Forward-Looking Prob PDFDrágus EmőkeNo ratings yet
- CT Image Quality FactorsDocument7 pagesCT Image Quality FactorsThome JerkNo ratings yet
- Sonopathology 1Document9 pagesSonopathology 1Ivette M. Carroll D.No ratings yet
- Nnano 2012 196Document2 pagesNnano 2012 196MardeySantanaNo ratings yet
- Radu. Strut Aposition After Coronary Stent Implantation Visualised With OCT. Eurointerv 2010Document8 pagesRadu. Strut Aposition After Coronary Stent Implantation Visualised With OCT. Eurointerv 2010Maria CardioNo ratings yet
- Qims 12 01 766Document15 pagesQims 12 01 766Hamza ArjahNo ratings yet
- Jurnal ReadingDocument7 pagesJurnal ReadingHanif UlinNo ratings yet
- Ultrasonic Imaging 13, 111-134 (1991) : AcademicDocument24 pagesUltrasonic Imaging 13, 111-134 (1991) : AcademicMR Emam - GamingNo ratings yet
- JPM 11 00515 v2Document25 pagesJPM 11 00515 v2Hasnain Ali ShahNo ratings yet
- Chondral Tumours - Discrepancy Rate Between Needle Biopsy and Surgical HistologyDocument11 pagesChondral Tumours - Discrepancy Rate Between Needle Biopsy and Surgical Histologychenth3r3No ratings yet
- Lamina Cribrosa Microarchitecture in Normal Monkey Eyes Part 1 Methods and Initial ResultsDocument20 pagesLamina Cribrosa Microarchitecture in Normal Monkey Eyes Part 1 Methods and Initial ResultskapilNo ratings yet
- Biomedics OpticsDocument6 pagesBiomedics OpticsazmatNo ratings yet
- Scientific Abstracts Friday, 14 June 2019 1015Document1 pageScientific Abstracts Friday, 14 June 2019 1015حسام الدين إسماعيلNo ratings yet
- Advances in Microscopy Techniques: Review ArticleDocument9 pagesAdvances in Microscopy Techniques: Review Articlekajol22fulNo ratings yet
- Oe 12 21 5178Document13 pagesOe 12 21 5178Fauzan AdamNo ratings yet
- Autoencoders - Bits and Bytes of Deep Learning - Towards Data ScienceDocument10 pagesAutoencoders - Bits and Bytes of Deep Learning - Towards Data ScienceMohit SinghNo ratings yet
- Unit 2 Classification of Parallel Computers: Structure NosDocument19 pagesUnit 2 Classification of Parallel Computers: Structure Nosjind_never_thinkNo ratings yet
- BookDocument133 pagesBookZhiMin ZongNo ratings yet
- Automatic Classification of Atherosclerotic Plaques Imaged With Intravascular OctDocument63 pagesAutomatic Classification of Atherosclerotic Plaques Imaged With Intravascular OctMohit SinghNo ratings yet
- BayesDocument9 pagesBayesSiddhesh ParabNo ratings yet
- Critique of Automatic Tissue CharacterizationDocument12 pagesCritique of Automatic Tissue CharacterizationMohit SinghNo ratings yet
- Computer - System - Architecture - 3rd - Ed - Morr Solution Mannual PDFDocument98 pagesComputer - System - Architecture - 3rd - Ed - Morr Solution Mannual PDFMohit SinghNo ratings yet
- Automatic Classification of AtheroscleroticDocument47 pagesAutomatic Classification of AtheroscleroticMohit SinghNo ratings yet
- An Adaptive Codebook Model For Change Detection With Dynamic BackgroundDocument7 pagesAn Adaptive Codebook Model For Change Detection With Dynamic BackgroundMohit SinghNo ratings yet
- JavaScript Course Notes PDFDocument130 pagesJavaScript Course Notes PDFsingyee123100% (1)
- Vbscript TutorialDocument191 pagesVbscript TutorialSandesh M MadkaikarNo ratings yet
- Cardiac Surgery in The Adult-3rd EditionDocument1,729 pagesCardiac Surgery in The Adult-3rd EditionFlorentina Negoita96% (26)
- Secondary Stroke PreventionDocument54 pagesSecondary Stroke PreventionHùng Phạm Lý ChíNo ratings yet
- Anatomy and Physiology of the HeartDocument56 pagesAnatomy and Physiology of the Heartamjad khan100% (1)
- PracticeExam 3 AnsDocument52 pagesPracticeExam 3 AnsBehrouz YariNo ratings yet
- Anandhi ResumeDocument7 pagesAnandhi ResumeAnonymous rMa4DVY5J2No ratings yet
- FREE 2021 ACLS Study Guide - ACLS Made Easy!Document32 pagesFREE 2021 ACLS Study Guide - ACLS Made Easy!Alen ArguellesNo ratings yet
- IsdnDocument5 pagesIsdnWidya JelitaNo ratings yet
- Exercise 10 The Lymphatic System: ZOO 115 Animal Histology Laboratory Exercises 1Document4 pagesExercise 10 The Lymphatic System: ZOO 115 Animal Histology Laboratory Exercises 1Christi Lorraine LayogNo ratings yet
- Deep Vein ThrombosisDocument3 pagesDeep Vein Thrombosisglenn johnston100% (1)
- Hypertension PathophysiologyDocument1 pageHypertension PathophysiologyTiffany Blanca Evangelista RaiNo ratings yet
- Dysrhythmia Interpretation Modules 1-6 June 2012Document126 pagesDysrhythmia Interpretation Modules 1-6 June 2012Jess Varose100% (3)
- Cor PulmonaleDocument14 pagesCor PulmonaleEvangelin MelvinNo ratings yet
- Study of Lipid Profile in Coronary Heart Disease Patients in LibyaDocument9 pagesStudy of Lipid Profile in Coronary Heart Disease Patients in LibyaInternational Medical PublisherNo ratings yet
- Atrial FibrillationDocument19 pagesAtrial FibrillationAnwari MuhammadNo ratings yet
- Updates American Heart Association Cardiopulmonary Resuscitation GuidelineDocument32 pagesUpdates American Heart Association Cardiopulmonary Resuscitation GuidelineramzishindiNo ratings yet
- Amity College of Nursing: Nursing Care Plan ON Heart FailureDocument20 pagesAmity College of Nursing: Nursing Care Plan ON Heart Failurejyoti puniaNo ratings yet
- Congenital Heart Disease - ASDDocument36 pagesCongenital Heart Disease - ASDAuni Akif Aleesa100% (1)
- Cardiac Arrest Case Report and CPR GuidelinesDocument50 pagesCardiac Arrest Case Report and CPR GuidelinesTajul AnshorNo ratings yet
- Cicrulatory and Immune Workbook KEYDocument32 pagesCicrulatory and Immune Workbook KEYgeorgia robinsonNo ratings yet
- Cardiovascular System-GlosaryDocument3 pagesCardiovascular System-GlosaryJennevi BrunoNo ratings yet
- Chronic Limb IschemiaDocument45 pagesChronic Limb IschemiaChristine TeNo ratings yet
- AcceptedDocument28 pagesAcceptedChistian LassoNo ratings yet
- Shock: Robert H. Sirait, DR.,SP An Dept. of Anesthesia FK UKI JakartaDocument22 pagesShock: Robert H. Sirait, DR.,SP An Dept. of Anesthesia FK UKI JakartaMuhammad Faisal AminNo ratings yet
- The History of Ecg MachineDocument4 pagesThe History of Ecg MachineAshley Nicole LimNo ratings yet
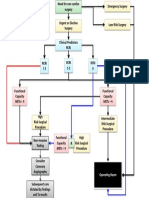
- Cardiac Risk Assessemnt FlowchartDocument1 pageCardiac Risk Assessemnt FlowchartjamesomooreNo ratings yet
- Principles and Pitfalls in Coronary Vasomotor Function TestingDocument26 pagesPrinciples and Pitfalls in Coronary Vasomotor Function TestingRamón López PalopNo ratings yet
- iGA Iforia-ProMRI Mul 393471-J 2017-11-24 EsDocument76 pagesiGA Iforia-ProMRI Mul 393471-J 2017-11-24 EsMartin ArrietaNo ratings yet
- A Case Study OnDocument176 pagesA Case Study OnTasneem MamokanNo ratings yet
- Septum Formation in The VentriclesDocument43 pagesSeptum Formation in The VentriclesAhsan IslamNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityFrom EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityRating: 4.5 out of 5 stars4.5/5 (109)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)