You might also like
- 04 Ifelse Return Input StringsDocument17 pages04 Ifelse Return Input StringsLhay DizonNo ratings yet
- 02 Expressions Variables ForloopsDocument15 pages02 Expressions Variables ForloopsLhay DizonNo ratings yet
- 03 Parameters GraphicsDocument19 pages03 Parameters GraphicsLhay DizonNo ratings yet
- IT 7 - Pendekatan Diagnostik Limfadenopati Limfadenitis - NDDocument46 pagesIT 7 - Pendekatan Diagnostik Limfadenopati Limfadenitis - NDRebeka Anastasia MarpaungNo ratings yet
- Gall StonesDocument26 pagesGall StonesNia SinghNo ratings yet
- HSC 2010 3.1 Week 1Document14 pagesHSC 2010 3.1 Week 1Andi Tenri PakkuaNo ratings yet
- USG Trimester 1 21-11-05Document78 pagesUSG Trimester 1 21-11-05nurmalidaseptiaNo ratings yet
- What's New in Cardiopulmonary BypassDocument31 pagesWhat's New in Cardiopulmonary Bypass凌晓敏No ratings yet
- Diagnosis and Management of Infantile HemangiomaDocument47 pagesDiagnosis and Management of Infantile HemangiomaSteph FergusonNo ratings yet
- (IJoC) Case Report TemplateDocument5 pages(IJoC) Case Report TemplateIren uhnanaNo ratings yet
- Konjungtivitis Dan KeratitisDocument117 pagesKonjungtivitis Dan KeratitisResti Puteri ApriyuslimNo ratings yet
- Repro & Endo 3Document26 pagesRepro & Endo 3abdulNo ratings yet
- Anterior Aspect of The Forearm Cubital Fossa 2012Document28 pagesAnterior Aspect of The Forearm Cubital Fossa 2012Elena IftimiNo ratings yet
- Dr. Imam Sofii Profile and Thyroid Nodule OverviewDocument18 pagesDr. Imam Sofii Profile and Thyroid Nodule OverviewRachman UsmanNo ratings yet
- Multidisciplinary Management of Gastroesophageal Reflux DiseaseDocument225 pagesMultidisciplinary Management of Gastroesophageal Reflux DiseaseCirjaliu Murgea MarinaNo ratings yet
- Radio Anatomy of The Thorax and Medias Tin Um 9-17Document113 pagesRadio Anatomy of The Thorax and Medias Tin Um 9-17Ditas ChuNo ratings yet
- CT Brain Part II-AnatomyDocument65 pagesCT Brain Part II-AnatomyXhenni XhenniNo ratings yet
- Buku - Abstract SymposiumDocument319 pagesBuku - Abstract SymposiumStephanie MurphyNo ratings yet
- DsaDocument25 pagesDsatcthanhNo ratings yet
- Anatomy of the Eye: Structures and FunctionsDocument29 pagesAnatomy of the Eye: Structures and FunctionsKiki Qurrotul Ayuni IINo ratings yet
- Overview of Neck Trauma: By: DR Noor Aneeza MD NoorDocument60 pagesOverview of Neck Trauma: By: DR Noor Aneeza MD NoorSaifizi SaidonNo ratings yet
- Boulevard of Broken Dreams LyricsDocument2 pagesBoulevard of Broken Dreams LyricsAlfonso Medina FriasNo ratings yet
- Aaron Cohen-Gadol CVDocument41 pagesAaron Cohen-Gadol CVBilly UntuNo ratings yet
- List of BooksDocument11 pagesList of Bookswefwewe3dsfNo ratings yet
- Nefrolitiasis RadiologiDocument9 pagesNefrolitiasis RadiologiSteven SetioNo ratings yet
- GraphPad Ebook - Essential Dos Don'TsDocument10 pagesGraphPad Ebook - Essential Dos Don'TsNikunj MittalNo ratings yet
- Dropped Nucleus ManagementDocument32 pagesDropped Nucleus ManagementNiloy Basak100% (2)
- Konsep EnsembleDocument52 pagesKonsep Ensemblehary170893No ratings yet
- Embriologi Ginjal dan PengembangannyaDocument39 pagesEmbriologi Ginjal dan PengembangannyaUttari DalemNo ratings yet
- Automated Image Detection of Retinal Pathology PDFDocument386 pagesAutomated Image Detection of Retinal Pathology PDFManish Mahabir0% (1)
- MATLAB - Application Used in Civil Engineering StructuresDocument4 pagesMATLAB - Application Used in Civil Engineering StructuresIJRASETPublicationsNo ratings yet
- MC Inauguration SampleDocument3 pagesMC Inauguration SampleSibi SanNo ratings yet
- Hypospadias: Case ReportDocument24 pagesHypospadias: Case Reportbudi haryadiNo ratings yet
- Referat Acute Liver FailureDocument124 pagesReferat Acute Liver FailurepanduNo ratings yet
- Thoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryDocument8 pagesThoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryIJAR JOURNALNo ratings yet
- Anterior Resection With Low AnastomosisDocument10 pagesAnterior Resection With Low AnastomosisOhana S.No ratings yet
- Pang ExpansionSphincter PDFDocument70 pagesPang ExpansionSphincter PDFIñaki ErdozáinNo ratings yet
- Early Pregnancy Bleeding Causes and TypesDocument14 pagesEarly Pregnancy Bleeding Causes and TypesMrs Rehan100% (1)
- Salman M., Roberto C. Heros, Edward R. Laws-Kempe's Operative Neurosurgery. Vol. I-II-Springer (2004)Document459 pagesSalman M., Roberto C. Heros, Edward R. Laws-Kempe's Operative Neurosurgery. Vol. I-II-Springer (2004)Silvia SanduNo ratings yet
- CC Radiology Physics JUN 2011Document38 pagesCC Radiology Physics JUN 2011Paris Revithis100% (1)
- Watery Eye: Magdy Fawzy $ Taha Sarhan Prof of OphthalmologyDocument93 pagesWatery Eye: Magdy Fawzy $ Taha Sarhan Prof of OphthalmologymiemednoteNo ratings yet
- CT For PE Breathing Technique PRESENTATIONDocument17 pagesCT For PE Breathing Technique PRESENTATIONEka JuliantaraNo ratings yet
- Intradural Extramedullary TumorsDocument10 pagesIntradural Extramedullary TumorsFaizyab AhmedNo ratings yet
- MR Okor SAC Neurosurgery CVDocument8 pagesMR Okor SAC Neurosurgery CVdrokor8747No ratings yet
- The Incidence, Risk Factors and Outcome of Retinopathy of Prematurity at A Tertiary Care Centre in South IndiaDocument7 pagesThe Incidence, Risk Factors and Outcome of Retinopathy of Prematurity at A Tertiary Care Centre in South IndiaIOSRjournalNo ratings yet
- Extention PDF Cath Lab TechDocument2 pagesExtention PDF Cath Lab TechChrisNo ratings yet
- Black Book CalgaryDocument386 pagesBlack Book CalgaryJackNo ratings yet
- Olanzapine Vs AripiprazoleDocument8 pagesOlanzapine Vs AripiprazoleDivaviyaNo ratings yet
- Jamur-Jamur Penyebab: Mikosis Superfisial Dermatofitosis Mikosis SubkutanDocument104 pagesJamur-Jamur Penyebab: Mikosis Superfisial Dermatofitosis Mikosis SubkutanJimmy Fran IINo ratings yet
- Papiledema 3Document27 pagesPapiledema 3nellieauthorNo ratings yet
- Reading A Head CT, What Every EP Should Know PDFDocument62 pagesReading A Head CT, What Every EP Should Know PDFAdistya Sari100% (1)
- Reading CT Scan of Human BrainDocument12 pagesReading CT Scan of Human BrainSumit RoyNo ratings yet
- P1Document12 pagesP1Roykedona Lisa TrixieNo ratings yet
- World Journal of Radiology PDFDocument8 pagesWorld Journal of Radiology PDFniluhNo ratings yet
- 39 MCQ's in NeurosurgeryDocument26 pages39 MCQ's in NeurosurgeryAhmed Hamid Ibrahim100% (4)
- Author's Accepted Manuscript: Seminars in Ultrasound, CT, and MRIDocument29 pagesAuthor's Accepted Manuscript: Seminars in Ultrasound, CT, and MRIasfwegereNo ratings yet
- CT Scan Head N BrainDocument45 pagesCT Scan Head N Brainaria tristayanthiNo ratings yet
- Head Trauma CT Scan Case StudyDocument8 pagesHead Trauma CT Scan Case Studytruevine_ministry100% (1)
- Neurosurgey MCQ Collection Part IDocument35 pagesNeurosurgey MCQ Collection Part IMohammed Ali Aldhahir88% (8)
- Neuro SurgeryDocument14 pagesNeuro Surgeryapi-3840195100% (4)
- (PAPAYA) Consolidated Manual Eng Ver0.5Document215 pages(PAPAYA) Consolidated Manual Eng Ver0.5Sergio MoradelNo ratings yet
- Iss Csi: Fujifilm DR SolutionDocument4 pagesIss Csi: Fujifilm DR Solutiond_abdosNo ratings yet
- LightSpeed 3.X Technical Reference Manual - UM - 2302180-100 - 8Document172 pagesLightSpeed 3.X Technical Reference Manual - UM - 2302180-100 - 8Ian Bruno Rodriguez CenturionNo ratings yet
- Problems and Solutions in Medical Physics DiagnosticDocument157 pagesProblems and Solutions in Medical Physics DiagnosticSubhrojitBagchiNo ratings yet
- Rotograph EVODocument11 pagesRotograph EVOLuis Fernando Garcia SanchezNo ratings yet
- PX-300HF,: 300ma Mobile X-Ray UnitDocument4 pagesPX-300HF,: 300ma Mobile X-Ray UnitRashid KhNo ratings yet
- Instruction ManualDocument137 pagesInstruction ManualKhalil IssaadNo ratings yet
- Heuft Spectrum: Modular HEUFT Systems of The New Generation. Highly Automated, Self-Explanatory andDocument9 pagesHeuft Spectrum: Modular HEUFT Systems of The New Generation. Highly Automated, Self-Explanatory andfernando betancourtNo ratings yet
- Radixray SPR CatálogoDocument28 pagesRadixray SPR CatálogoAlber Lim GboNo ratings yet
- Role of Inspection During The Lifetime of A PipelineDocument27 pagesRole of Inspection During The Lifetime of A Pipelinediaccessltd_17172961No ratings yet
- S. C. Bott Et Al - Study of The Effect of Current Rise Time On The Formation of The Precursor Column in Cylindrical Wire Array Z Pinches at 1 MADocument14 pagesS. C. Bott Et Al - Study of The Effect of Current Rise Time On The Formation of The Precursor Column in Cylindrical Wire Array Z Pinches at 1 MACola7890No ratings yet
- Brilliance CT: 6-Slice, 10-Slice, 16-Slice, and 16 Power ConfigurationsDocument66 pagesBrilliance CT: 6-Slice, 10-Slice, 16-Slice, and 16 Power ConfigurationsdanielNo ratings yet
- Science 10 Module 3Document8 pagesScience 10 Module 3RODJHEN ANNE P. BARQUILLANo ratings yet
- Introduction To Radiology: Dr. Wala Issa Bani Hamad M.D JBRDocument33 pagesIntroduction To Radiology: Dr. Wala Issa Bani Hamad M.D JBRAbdulrahman AlsayyedNo ratings yet
- Xray Kub My Prep FinalDocument109 pagesXray Kub My Prep FinalphoenixibexNo ratings yet
- Safety Dental PracticeDocument11 pagesSafety Dental PracticeEking InNo ratings yet
- Sensometry, Xray Film and Intensifying ScreensDocument53 pagesSensometry, Xray Film and Intensifying ScreensFrank OpiyoNo ratings yet
- Radiographic Positioning DogDocument1 pageRadiographic Positioning DogElena Martínez Celis100% (2)
- Training Manual Radiation Hazard Control in Industrial RadiographyDocument96 pagesTraining Manual Radiation Hazard Control in Industrial RadiographyBagiyono BagiyonoNo ratings yet
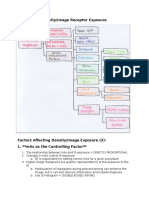
- Chapter 26: Density/Image Receptor Exposure: Notebook #7Document8 pagesChapter 26: Density/Image Receptor Exposure: Notebook #7api-338781568No ratings yet
- FUJİ CR Users-GuideDocument40 pagesFUJİ CR Users-Guideyekta8No ratings yet
- PX 6.4 English Product Brochure (PX6.4 - PB - 10APR12revF - PF)Document4 pagesPX 6.4 English Product Brochure (PX6.4 - PB - 10APR12revF - PF)Charles LiNo ratings yet
- Platinum Notes - RadiologyDocument40 pagesPlatinum Notes - RadiologyskNo ratings yet
- SDX 5000 - Operational ManuelDocument73 pagesSDX 5000 - Operational Manuelmelihayanoglu34No ratings yet
- AMT-Master Catalog FinalDocument32 pagesAMT-Master Catalog FinalamtdentalNo ratings yet
- XIS 6040 Tech Spec RevADocument16 pagesXIS 6040 Tech Spec RevAPaolo Coronado100% (2)
- X-Ray Diffraction Techniques For Soil Mineral IdentificationDocument36 pagesX-Ray Diffraction Techniques For Soil Mineral Identificationlimlerian100% (2)
- Radiographic 2 Previous Question PapersDocument6 pagesRadiographic 2 Previous Question PapersMahesh BodaNo ratings yet