You might also like
- Lesson 3 - Materials That Undergo DecayDocument14 pagesLesson 3 - Materials That Undergo DecayFUMIKO SOPHIA67% (6)
- Crossfit Level One Study GuideDocument115 pagesCrossfit Level One Study GuideJohn Warchild100% (2)
- Sap Ewm - Erp Initial SetupDocument3 pagesSap Ewm - Erp Initial SetupVAIBHAV PARAB80% (5)
- STS Chapter 5Document2 pagesSTS Chapter 5Cristine Laluna92% (38)
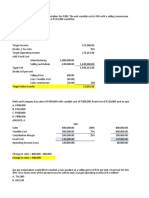
- CVP Solution (Quiz)Document9 pagesCVP Solution (Quiz)Angela Miles DizonNo ratings yet
- Blood Pressure Management in Patients With DiabetesDocument8 pagesBlood Pressure Management in Patients With DiabetesHoài ThươngNo ratings yet
- New Frontiers Hipertensi Part2Document8 pagesNew Frontiers Hipertensi Part2Eunike_oisNo ratings yet
- Cardiovascular Disease and Risk Management: American Diabetes AssociationDocument9 pagesCardiovascular Disease and Risk Management: American Diabetes AssociationIngrid DCNo ratings yet
- 27 FullDocument6 pages27 FullKrishna R KhanalNo ratings yet
- Hypertension in People With Type 2 DiabetesDocument6 pagesHypertension in People With Type 2 DiabetesIgor CampanaNo ratings yet
- DerosaDocument13 pagesDerosaAmeliana KamaludinNo ratings yet
- Accord StudyDocument2 pagesAccord StudyCarlos Danilo Noroña CNo ratings yet
- Blood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlDocument8 pagesBlood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlNovita WulandariNo ratings yet
- CCRR 1 114 PDFDocument3 pagesCCRR 1 114 PDFBruno Mario AngelNo ratings yet
- Hypertension in Diabetes: Treatment Considerations: Review PaperDocument5 pagesHypertension in Diabetes: Treatment Considerations: Review Paperdivina_grace08No ratings yet
- 2016 - Potential Drug Combinations To Reduce Cardiovascular Disease Burden in DiabetesDocument13 pages2016 - Potential Drug Combinations To Reduce Cardiovascular Disease Burden in DiabetesWENDY JOHANA HENRIQUEZ SEGURA ESTUDIANTE ACTIVONo ratings yet
- Diabetes and Cardiovascular DiseaseDocument119 pagesDiabetes and Cardiovascular DiseaseAlina PopaNo ratings yet
- Dyslipidemia in Diabetes Mellitus and Cardiovascular DiseaseDocument6 pagesDyslipidemia in Diabetes Mellitus and Cardiovascular DiseaseEward Rod SalNo ratings yet
- Kelompok 1Document14 pagesKelompok 1Aurent WidjanarkoNo ratings yet
- Cardiovascular Safety Profile of Currently Available Diabetic DrugsDocument17 pagesCardiovascular Safety Profile of Currently Available Diabetic Drugsvina_nursyaidahNo ratings yet
- Hta TtoDocument13 pagesHta TtoAmelia RiveraNo ratings yet
- 01 Hyp 37 4 1053Document7 pages01 Hyp 37 4 1053AuliaNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- Manage Dyslipidemia Adults DiabetesDocument4 pagesManage Dyslipidemia Adults DiabetesWahyuningsih HamidNo ratings yet
- Pharmacological Treatment of HyperlipiedmiaDocument8 pagesPharmacological Treatment of HyperlipiedmiajeffaguilarNo ratings yet
- 2017 Guideline For The Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults - Key Point To RememberDocument6 pages2017 Guideline For The Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults - Key Point To RememberSandy Kartika PurnomoNo ratings yet
- Perspective: Management of Hypertension in Patients With Type 2 Diabetes Mellitus: Guidelines Based On Current EvidenceDocument6 pagesPerspective: Management of Hypertension in Patients With Type 2 Diabetes Mellitus: Guidelines Based On Current EvidencethaihavttNo ratings yet
- ACCORD Trial Updates Blood Sugar, Pressure, Lipid ResultsDocument3 pagesACCORD Trial Updates Blood Sugar, Pressure, Lipid ResultsTyler HoffmanNo ratings yet
- Heart Failure The Frequent Forgotten and Often Fatal Complication of DiabetesDocument9 pagesHeart Failure The Frequent Forgotten and Often Fatal Complication of DiabetesMuinimula aluminiuM (MuminiminimuM)No ratings yet
- Diabetes and Hypertension: A Comprehensive Report On Management and The Prevention of Cardiovascular and Renal ComplicationsDocument3 pagesDiabetes and Hypertension: A Comprehensive Report On Management and The Prevention of Cardiovascular and Renal Complicationsrizqi_cepiNo ratings yet
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- HTA CanadaDocument3 pagesHTA Canadavasarhely imolaNo ratings yet
- Prediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DDocument9 pagesPrediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DCharlotte KeckhutNo ratings yet
- ADVANCE: Action in Diabetes and Vascular Disease: Original ArticleDocument6 pagesADVANCE: Action in Diabetes and Vascular Disease: Original ArticleMade LascanoNo ratings yet
- Use of Statins and The Incidence of Type 2 Diabetes MellitusDocument6 pagesUse of Statins and The Incidence of Type 2 Diabetes MellitusBenji MincholaNo ratings yet
- Interpretation of Cardiovascular Outcome TrialsDocument9 pagesInterpretation of Cardiovascular Outcome TrialsmagreaNo ratings yet
- Eso Beta BlokerDocument15 pagesEso Beta BlokerCarolina NauNo ratings yet
- Pavlou 2018Document7 pagesPavlou 2018anita putriNo ratings yet
- Case Study: 52-Year-Old Woman With Chest PainDocument4 pagesCase Study: 52-Year-Old Woman With Chest Painflex gyNo ratings yet
- PIIS0140673621023400Document2 pagesPIIS0140673621023400choirul anamNo ratings yet
- 2017 Guideline For High Blood Pressure in Adults - American College of Cardiology-Key PointsDocument7 pages2017 Guideline For High Blood Pressure in Adults - American College of Cardiology-Key PointsRahaf K. IbrahimNo ratings yet
- s80 FullDocument3 pagess80 FullDiego OrtechoNo ratings yet
- Case Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryDocument9 pagesCase Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryJohn PauloNo ratings yet
- Macroangiopatias DiabetesDocument16 pagesMacroangiopatias DiabetesJorge SolisNo ratings yet
- Thiazides and Diabetes: Pharmacist'S Letter / Prescriber'S LetterDocument2 pagesThiazides and Diabetes: Pharmacist'S Letter / Prescriber'S Lettercarramrod2No ratings yet
- Barrios Et Al. The LAURA Study. Int J Clin Pract 2006Document7 pagesBarrios Et Al. The LAURA Study. Int J Clin Pract 2006Ruth RachmawatyNo ratings yet
- Fixed Combinations in The Management OLM+AmloDocument12 pagesFixed Combinations in The Management OLM+AmloSherif AwadNo ratings yet
- Reading WK 3 PrisantDocument7 pagesReading WK 3 PrisantNur Laila SafitriNo ratings yet
- JournalDocument2 pagesJournalMichael FangkiNo ratings yet
- Case Study: Treating Hypertension in Patients With DiabetesDocument10 pagesCase Study: Treating Hypertension in Patients With Diabetesfirda rydNo ratings yet
- Case Studies in Hyperlipidemia: Michael Cobble, MD, FNLADocument6 pagesCase Studies in Hyperlipidemia: Michael Cobble, MD, FNLAKhánh ChiNo ratings yet
- Reviews: Statins in The Primary Prevention of Cardiovascular DiseaseDocument12 pagesReviews: Statins in The Primary Prevention of Cardiovascular DiseaseCrischentian BrinzaNo ratings yet
- Clinical Case Studies: Management of Dyslipidemia in Type 2 Diabetic Patient: A Case ReportDocument3 pagesClinical Case Studies: Management of Dyslipidemia in Type 2 Diabetic Patient: A Case ReportBaek ShinNo ratings yet
- Atherogenic Dyslipidemia in Patients With Established Coronary Artery DiseaseDocument6 pagesAtherogenic Dyslipidemia in Patients With Established Coronary Artery DiseasebilahalvirayuNo ratings yet
- HHF 9 E002560Document12 pagesHHF 9 E002560Putri Atthariq IlmiNo ratings yet
- Hypertension: A Focus On JNC VIIDocument95 pagesHypertension: A Focus On JNC VIITri GumilarNo ratings yet
- Terjemahan JurnalDocument13 pagesTerjemahan JurnalIqhe Harsono SyastrowinotoNo ratings yet
- Weight Loss Drug Cutting Risk of Heart AttackDocument12 pagesWeight Loss Drug Cutting Risk of Heart AttackWKYC.comNo ratings yet
- New England Journal Medicine: The ofDocument5 pagesNew England Journal Medicine: The ofAri Hidriansyah AtmajaNo ratings yet
- Ades-The Treatment of Obesity in Cardiac Rehabilitation 2021Document7 pagesAdes-The Treatment of Obesity in Cardiac Rehabilitation 2021markwsheppardhotmail.comNo ratings yet
- Antihypertensive Drug Class Interactions and Risk For Incident Diabetes: A Nested Case - Control StudyDocument9 pagesAntihypertensive Drug Class Interactions and Risk For Incident Diabetes: A Nested Case - Control StudylalaNo ratings yet
- 2018-10-31 Final Research Paper MPI CAD Vs HBA1CDocument12 pages2018-10-31 Final Research Paper MPI CAD Vs HBA1Cbilly medinaNo ratings yet
- 1 s2.0 S0002870320302143 MainDocument9 pages1 s2.0 S0002870320302143 MaindeepNo ratings yet
- Treatment of Cholesterol in 2017Document2 pagesTreatment of Cholesterol in 2017Bruno Andre Garcia VegaNo ratings yet
- Returning To Physical Activity After Covid-19Document6 pagesReturning To Physical Activity After Covid-19bacharelado2010No ratings yet
- LIU - Venovenous Extra-Corporeal Membrane Oxygenation For Severe AcuteDocument7 pagesLIU - Venovenous Extra-Corporeal Membrane Oxygenation For Severe Acutebacharelado2010No ratings yet
- Guidelines Extracorporeal Membrane Oxygenation For COVID-19Document11 pagesGuidelines Extracorporeal Membrane Oxygenation For COVID-19bacharelado2010No ratings yet
- Six-Month Survival After Extracorporeal Membrane Oxygenation For Severe COVID-19Document8 pagesSix-Month Survival After Extracorporeal Membrane Oxygenation For Severe COVID-19Alvaro EstupiñanNo ratings yet
- Survival Benefits of Extracorporeal Membrane OxygenationDocument5 pagesSurvival Benefits of Extracorporeal Membrane Oxygenationbacharelado2010No ratings yet
- Rehabilitation of Patients post-COVID-19 Infection: A Literature ReviewDocument10 pagesRehabilitation of Patients post-COVID-19 Infection: A Literature ReviewBastian AgungNo ratings yet
- UK Chief Medical Officers' Physical Activity Guidelines PDFDocument66 pagesUK Chief Medical Officers' Physical Activity Guidelines PDFCarolina PaezNo ratings yet
- Delivering Extracorporeal Membrane Oxygenation ForDocument5 pagesDelivering Extracorporeal Membrane Oxygenation Forbacharelado2010No ratings yet
- Returning To Physical Activity After Covid-19Document6 pagesReturning To Physical Activity After Covid-19bacharelado2010No ratings yet
- Mechanisms of Muscle HypertrophyDocument3 pagesMechanisms of Muscle Hypertrophybacharelado2010No ratings yet
- The Concept of Iso-Inertial AssessmentDocument10 pagesThe Concept of Iso-Inertial Assessmentbacharelado2010No ratings yet
- Conventional and Genetic Talent Identification in SportsDocument15 pagesConventional and Genetic Talent Identification in Sportsbacharelado2010No ratings yet
- A Prática de Exercícios Físicos É Um Fator Modificavel Da Incontinencia Urinaria de Urgencia em Mulheres IdosasDocument17 pagesA Prática de Exercícios Físicos É Um Fator Modificavel Da Incontinencia Urinaria de Urgencia em Mulheres Idosasbacharelado2010No ratings yet
- Body Composition and Fitness in Elite Spanish ChildrenDocument15 pagesBody Composition and Fitness in Elite Spanish Childrenbacharelado2010No ratings yet
- 6 Week Training Junior Program TennisDocument11 pages6 Week Training Junior Program TennisCiprianTeleaga0% (1)
- Agility Training: First StepDocument5 pagesAgility Training: First Stepbacharelado2010No ratings yet
- Cross Fit Journal PDFDocument11 pagesCross Fit Journal PDFPaulo TsunetaNo ratings yet
- Teorisa Se Tecnicas de MassagemDocument2 pagesTeorisa Se Tecnicas de Massagembacharelado2010No ratings yet
- Compendium of Physical Activities PDFDocument20 pagesCompendium of Physical Activities PDFJMedeirosNo ratings yet
- Conventional and Genetic Talent Identification in SportsDocument15 pagesConventional and Genetic Talent Identification in Sportsbacharelado2010No ratings yet
- Mechanisms of Muscle HypertrophyDocument16 pagesMechanisms of Muscle HypertrophySpongebob57100% (1)
- High Intensity Interval Training Efficient,.3Document1 pageHigh Intensity Interval Training Efficient,.3bacharelado2010No ratings yet
- High Intensity Interval Training Efficient,.3Document1 pageHigh Intensity Interval Training Efficient,.3bacharelado2010No ratings yet
- (R) - Checklist 6 Pontos ChaveDocument10 pages(R) - Checklist 6 Pontos ChaveJean Freitas LimaNo ratings yet
- Worldwide Survey of Fitness Trends For 2019.6Document8 pagesWorldwide Survey of Fitness Trends For 2019.6bacharelado2010100% (1)
- High Intensity Interval TrainingDocument2 pagesHigh Intensity Interval TrainingmilleralselmoNo ratings yet
- Hans SelyeDocument10 pagesHans SelyeZeyrra Mariana100% (2)
- Worldwide Survey of Fitness Trends For 2019.6Document8 pagesWorldwide Survey of Fitness Trends For 2019.6bacharelado2010100% (1)
- Impact of Healthy Lifestyle Factors On LifeDocument11 pagesImpact of Healthy Lifestyle Factors On Lifebacharelado2010No ratings yet
- Cantilever Retaining Wall AnalysisDocument7 pagesCantilever Retaining Wall AnalysisChub BokingoNo ratings yet
- Broadband BillDocument1 pageBroadband BillKushi GowdaNo ratings yet
- DX133 DX Zero Hair HRL Regular 200 ML SDS 16.04.2018 2023Document6 pagesDX133 DX Zero Hair HRL Regular 200 ML SDS 16.04.2018 2023Welissa ChicanequissoNo ratings yet
- Norms and specifications for distribution transformer, DG set, street light poles, LED lights and high mast lightDocument4 pagesNorms and specifications for distribution transformer, DG set, street light poles, LED lights and high mast lightKumar AvinashNo ratings yet
- Feb 22-Additional CasesDocument27 pagesFeb 22-Additional CasesYodh Jamin OngNo ratings yet
- Exam Venue For Monday Sep 25, 2023 - 12-00 To 01-00Document7 pagesExam Venue For Monday Sep 25, 2023 - 12-00 To 01-00naveed hassanNo ratings yet
- BUSN7054 Take Home Final Exam S1 2020Document14 pagesBUSN7054 Take Home Final Exam S1 2020Li XiangNo ratings yet
- UNIT: 01 Housekeeping SupervisionDocument91 pagesUNIT: 01 Housekeeping SupervisionRamkumar RamkumarNo ratings yet
- MTS Material Testing SolutionsDocument34 pagesMTS Material Testing SolutionskarthegreNo ratings yet
- Marketing Management NotesDocument115 pagesMarketing Management NotesKajwangs DanNo ratings yet
- Easyjet Group6Document11 pagesEasyjet Group6Rishabh RakhechaNo ratings yet
- SEEPZ Special Economic ZoneDocument2 pagesSEEPZ Special Economic ZonetarachandmaraNo ratings yet
- Part 9. Wireless Communication Towers and Antennas 908.01 Purpose and IntentDocument12 pagesPart 9. Wireless Communication Towers and Antennas 908.01 Purpose and IntentjosethompsonNo ratings yet
- Terminología Sobre Reducción de Riesgo de DesastresDocument43 pagesTerminología Sobre Reducción de Riesgo de DesastresJ. Mario VeraNo ratings yet
- Equity AdvisorDocument2 pagesEquity AdvisorHarshit AgarwalNo ratings yet
- JWCh06 PDFDocument23 pagesJWCh06 PDF007featherNo ratings yet
- BIU and EU functions in 8086 microprocessorDocument12 pagesBIU and EU functions in 8086 microprocessorDaksh ShahNo ratings yet
- Fleck 3150 Downflow: Service ManualDocument40 pagesFleck 3150 Downflow: Service ManualLund2016No ratings yet
- Leapfroggers, People Who Start A Company, Manage Its Growth Until They Get Bored, and Then SellDocument3 pagesLeapfroggers, People Who Start A Company, Manage Its Growth Until They Get Bored, and Then Sellayesha noorNo ratings yet
- Eship 1Document18 pagesEship 1Yash SoniNo ratings yet
- Chirala, Andhra PradeshDocument7 pagesChirala, Andhra PradeshRam KumarNo ratings yet
- Statement of PurposeDocument2 pagesStatement of Purposearmaan kaurNo ratings yet
- A K A G .: RUN Umar Shok UptaDocument2 pagesA K A G .: RUN Umar Shok UptaArun GuptaNo ratings yet
- NH School Employee Criminal Record Check FormDocument2 pagesNH School Employee Criminal Record Check FormEmily LescatreNo ratings yet
- WPB Pitch DeckDocument20 pagesWPB Pitch Deckapi-102659575No ratings yet
- Ultrasonic Examination of Heavy Steel Forgings: Standard Practice ForDocument7 pagesUltrasonic Examination of Heavy Steel Forgings: Standard Practice ForbatataNo ratings yet