You might also like
- Before The Judge - Roger EDocument26 pagesBefore The Judge - Roger ELexLuther1776100% (4)
- Assessment of Nutritional Status of Under Five Children Attending Post Natal Clinic at OjaDocument35 pagesAssessment of Nutritional Status of Under Five Children Attending Post Natal Clinic at OjaOpeyemi JamalNo ratings yet
- Nutritional Assessment Lecture 1Document28 pagesNutritional Assessment Lecture 1ESUFIYAN ALWSABINo ratings yet
- Research Proposal ExampleDocument3 pagesResearch Proposal Exampleapi-339321505100% (1)
- Annotated Bibliography DraftDocument13 pagesAnnotated Bibliography Draftapi-252551056No ratings yet
- Nutrition and Students Academic PerformanceDocument10 pagesNutrition and Students Academic Performanceapi-222239614No ratings yet
- Health Situational AnalysisDocument70 pagesHealth Situational AnalysisGretchen Mae Corrales100% (1)
- MALNUTRITIONDocument30 pagesMALNUTRITIONbrian sam100% (2)
- Nurtition Across The LifespanDocument11 pagesNurtition Across The LifespanFrancel Zyrene LabaoNo ratings yet
- CHAPTER 1 - 3 Q Flashcards - QuizletDocument17 pagesCHAPTER 1 - 3 Q Flashcards - Quizletrochacold100% (1)
- DepEd Red Cross 3 4 Seater Detached PoWs BoQsDocument42 pagesDepEd Red Cross 3 4 Seater Detached PoWs BoQsRamil S. ArtatesNo ratings yet
- Project Proposal On Child Nutrition For Sustainable Health and Prenatal ClinicDocument5 pagesProject Proposal On Child Nutrition For Sustainable Health and Prenatal Clinicczeremar chan0% (1)
- City Nutrition Scholar Consolidated Annual Accpomplishment Report TemplateDocument7 pagesCity Nutrition Scholar Consolidated Annual Accpomplishment Report TemplateBarangay Sudlon 1No ratings yet
- MalnutritionDocument5 pagesMalnutritionPhOebe Soliven GabrielNo ratings yet
- Prevalence of Malnutrition at Aleta Chuko Town, SNNPR, Ethiopia, DR Kassahun Girma Et. AlDocument45 pagesPrevalence of Malnutrition at Aleta Chuko Town, SNNPR, Ethiopia, DR Kassahun Girma Et. AlKassahun Girma Gelaw67% (3)
- Compilation of Nutri Ed ProgramsDocument5 pagesCompilation of Nutri Ed ProgramsDarwell Chann RosalesNo ratings yet
- UNICEF Conceptual Framework of MalnutritionDocument4 pagesUNICEF Conceptual Framework of MalnutritionAyu Putri Noviyanti100% (2)
- PCOS: Raising Awareness and Empowering WomenDocument29 pagesPCOS: Raising Awareness and Empowering WomenShantanu Nair100% (1)
- Annotated BibliographyDocument7 pagesAnnotated Bibliographyapi-302552436No ratings yet
- CompTIA Network+Document3 pagesCompTIA Network+homsom100% (1)
- SOCIAL CLASS DIFFERENCES IN FOOD CONSUMPTION BarkiDocument32 pagesSOCIAL CLASS DIFFERENCES IN FOOD CONSUMPTION BarkiSumaiya AlviNo ratings yet
- Malnutrition FinalDocument66 pagesMalnutrition FinalAmit Pasi100% (2)
- Exclusive BreastfeedingDocument19 pagesExclusive BreastfeedingVANGAWA JOHNNo ratings yet
- Community Project PlanDocument13 pagesCommunity Project PlanMizuiro SenpaiNo ratings yet
- Chapter 1-3Document81 pagesChapter 1-3Jewelle Ann AlanisNo ratings yet
- Chapter 1 5 Super FinalOther ResearchDocument176 pagesChapter 1 5 Super FinalOther ResearchjeffreyNo ratings yet
- Factors Associated With Under Nutrition in Children Under Five Years in Bangaladesh Parish, Namasale Sub-County, Amolatar DistrictDocument10 pagesFactors Associated With Under Nutrition in Children Under Five Years in Bangaladesh Parish, Namasale Sub-County, Amolatar DistrictKIU PUBLICATION AND EXTENSION100% (1)
- Factors Related To Malnutrition Among Children Below Five Years in Rengen Health Center III, Kotido DistrictDocument13 pagesFactors Related To Malnutrition Among Children Below Five Years in Rengen Health Center III, Kotido DistrictKIU PUBLICATION AND EXTENSION100% (1)
- Research Abstracts On NutritionDocument172 pagesResearch Abstracts On NutritionKulwinder KaurNo ratings yet
- Factors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaDocument10 pagesFactors Influencing Malnutrition Among Under Five Children at Kitwe Teaching Hospital, ZambiaInternational Journal of Current Innovations in Advanced Research100% (1)
- Tembo Precious ProposalDocument13 pagesTembo Precious ProposalEvangelist Kabaso SydneyNo ratings yet
- Chapter 1 RevsionDocument22 pagesChapter 1 RevsionLyn ErnieNo ratings yet
- ABDURRAHIMTPDocument32 pagesABDURRAHIMTPUsman Ahmad TijjaniNo ratings yet
- Impact of Television On Eating Habits of School Going ChildrenDocument5 pagesImpact of Television On Eating Habits of School Going ChildrenIJRASETPublications100% (1)
- FINAL 2018 Nutrition Month Talking Points PDFDocument36 pagesFINAL 2018 Nutrition Month Talking Points PDFLubeth Cabatu100% (3)
- Factors Affecting Developmental Milestones Among Children Under Five Years Attending Child Welfare Clinic in Nyamira County Referral Hospital.Document27 pagesFactors Affecting Developmental Milestones Among Children Under Five Years Attending Child Welfare Clinic in Nyamira County Referral Hospital.Joshua MokayaNo ratings yet
- Statement of The ProblemDocument13 pagesStatement of The ProblemDaniel LeoNo ratings yet
- NSTP Project ProposalDocument15 pagesNSTP Project ProposalleighNo ratings yet
- Review of Related LiteratureDocument4 pagesReview of Related LiteratureJessica Cabildo CalbanNo ratings yet
- Effects of Malnutrition Among ChildrenDocument3 pagesEffects of Malnutrition Among ChildrenDesiree Aranggo MangueraNo ratings yet
- 7th National Nutrition SurveyDocument2 pages7th National Nutrition SurveyJorace VillamilNo ratings yet
- Nutritional Status of Adolescent School GirlsDocument126 pagesNutritional Status of Adolescent School GirlsArshad Mahmood Uppal71% (7)
- Integrated Midwives Association of The Philippines (Imap) Foundation School of Midwifery, IncDocument43 pagesIntegrated Midwives Association of The Philippines (Imap) Foundation School of Midwifery, IncFhikery ArdienteNo ratings yet
- Suplementary Feeding (C)Document19 pagesSuplementary Feeding (C)Dyiana Mhay JunioNo ratings yet
- 2016 Nutrition Month Talking PointsDocument28 pages2016 Nutrition Month Talking PointsEli Benjamin Nava Taclino89% (9)
- IRC Kenya - Reducing Malnutrition in Hagadera and Kakuma Camps (2011)Document26 pagesIRC Kenya - Reducing Malnutrition in Hagadera and Kakuma Camps (2011)Matija KovacNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument27 pagesRajiv Gandhi University of Health Sciences Bangalore, Karnatakasathyasai999No ratings yet
- Report ICDS PDFDocument119 pagesReport ICDS PDFSaleem MalikNo ratings yet
- School Feeding ProgramDocument2 pagesSchool Feeding ProgramJEZANAIHNo ratings yet
- Chapter-2 Hunger and Malnutrition in India - Policies and ProgrammesDocument35 pagesChapter-2 Hunger and Malnutrition in India - Policies and ProgrammesJames KnotNo ratings yet
- National Nutrition Programm and PolicyDocument15 pagesNational Nutrition Programm and PolicyDr.ekta singh chauhan100% (1)
- Adolescent Nutrition Intervention Guideline 3rd Draft July 20221Document79 pagesAdolescent Nutrition Intervention Guideline 3rd Draft July 20221Edris Abdella Nuure100% (1)
- Assessment of Nutrition Profile of Pregnant Women in Rural Area (Mymensingh District) of BangladeshDocument6 pagesAssessment of Nutrition Profile of Pregnant Women in Rural Area (Mymensingh District) of BangladeshKanhiya MahourNo ratings yet
- Garantisadong PambataDocument6 pagesGarantisadong PambatasweetyjonasNo ratings yet
- Office Secretary: Administrative 0055 Subject: National Guidelines ForDocument19 pagesOffice Secretary: Administrative 0055 Subject: National Guidelines ForJonathan Renier Verzosa0% (1)
- Sample Meal Plan For Feeding Your PreschoolerDocument8 pagesSample Meal Plan For Feeding Your PreschoolerJack ParungaoNo ratings yet
- Nutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanDocument5 pagesNutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanIjaems JournalNo ratings yet
- A Study To Assess Knowledge and Awareness About The HIVAIDS Among StudentsDocument7 pagesA Study To Assess Knowledge and Awareness About The HIVAIDS Among StudentsAMALIA PEBRIYANTINo ratings yet
- Infant and Young Feeding ProgramDocument23 pagesInfant and Young Feeding ProgramAnonymous Gwa6bMNo ratings yet
- Plan of Action NutritionDocument31 pagesPlan of Action NutritionMary Rose MartinezNo ratings yet
- Nutritional Intake Among Older People of Hermana Fausta Development Center, Lucena City and Its Relationship To Physical Health StatusDocument20 pagesNutritional Intake Among Older People of Hermana Fausta Development Center, Lucena City and Its Relationship To Physical Health StatusAngelNo ratings yet
- A Case Study of Polycystic Ovarian SyndromeDocument42 pagesA Case Study of Polycystic Ovarian SyndromeDORINNE KINDAONo ratings yet
- RESEARCH093016Document28 pagesRESEARCH093016Satra Sabbuh100% (1)
- Coursework Assignment: Graduate Job ImpactDocument13 pagesCoursework Assignment: Graduate Job ImpactmirwaisNo ratings yet
- Hunting the Chimera–the end of O'Reilly v Mackman_ -- Alder, John -- Legal Studies, #2, 13, pages 183-20...hn Wiley and Sons; Cambridge -- 10_1111_j_1748-121x_1993_tb00480_x -- 130f73b26a9d16510be20781ea4d81eb -- Anna’s ArchiveDocument21 pagesHunting the Chimera–the end of O'Reilly v Mackman_ -- Alder, John -- Legal Studies, #2, 13, pages 183-20...hn Wiley and Sons; Cambridge -- 10_1111_j_1748-121x_1993_tb00480_x -- 130f73b26a9d16510be20781ea4d81eb -- Anna’s ArchivePrince KatheweraNo ratings yet
- Unit Test 11 PDFDocument1 pageUnit Test 11 PDFYONo ratings yet
- Brunon BradDocument2 pagesBrunon BradAdamNo ratings yet
- SiswaDocument5 pagesSiswaNurkholis MajidNo ratings yet
- CMAT Score CardDocument1 pageCMAT Score CardRaksha RudraNo ratings yet
- TRB - HSK NC IiiDocument7 pagesTRB - HSK NC IiiBlessy AlinaNo ratings yet
- Service Letter SL2019-672/CHSO: PMI Sensor Calibration RequirementsDocument3 pagesService Letter SL2019-672/CHSO: PMI Sensor Calibration RequirementsSriram SridharNo ratings yet
- Au L 53229 Introduction To Persuasive Text Powerpoint - Ver - 1Document13 pagesAu L 53229 Introduction To Persuasive Text Powerpoint - Ver - 1Gacha Path:3No ratings yet
- Times Leader 03-16-2013Document61 pagesTimes Leader 03-16-2013The Times LeaderNo ratings yet
- Beowulf Essay 1Document6 pagesBeowulf Essay 1api-496952332No ratings yet
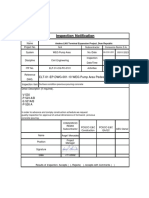
- In-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsDocument5 pagesIn-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsPedro PaulinoNo ratings yet
- BLR - Overall Attendance Report - 22mar24Document64 pagesBLR - Overall Attendance Report - 22mar24Purahar sathyaNo ratings yet
- API1 2019 Broken Object Level AuthorizationDocument7 pagesAPI1 2019 Broken Object Level AuthorizationShamsher KhanNo ratings yet
- Final Draft RTS On SADocument84 pagesFinal Draft RTS On SAjose pazNo ratings yet
- D Matei About The Castra in Dacia and THDocument22 pagesD Matei About The Castra in Dacia and THBritta BurkhardtNo ratings yet
- CT 1 - QP - Icse - X - GSTDocument2 pagesCT 1 - QP - Icse - X - GSTAnanya IyerNo ratings yet
- Cuthites: Cuthites in Jewish LiteratureDocument2 pagesCuthites: Cuthites in Jewish LiteratureErdincNo ratings yet
- .. Anadolu Teknik, Teknik Lise Ve Endüstri Meslek LisesiDocument3 pages.. Anadolu Teknik, Teknik Lise Ve Endüstri Meslek LisesiLisleNo ratings yet
- Student Guidelines The School PoliciesDocument5 pagesStudent Guidelines The School PoliciesMaritessNo ratings yet
- Philippine National Development Goals Vis-A-Vis The Theories and Concepts of Public Administration and Their Applications.Document2 pagesPhilippine National Development Goals Vis-A-Vis The Theories and Concepts of Public Administration and Their Applications.Christian LeijNo ratings yet
- Pineapples Export's To Copenhagen, DenmarkDocument13 pagesPineapples Export's To Copenhagen, DenmarkMuhammad SyafiqNo ratings yet
- ThesisDocument44 pagesThesisjagritiNo ratings yet
- Financial Amendment Form: 1 General InformationDocument3 pagesFinancial Amendment Form: 1 General InformationRandolph QuilingNo ratings yet
- GHMC Results, 2009Document149 pagesGHMC Results, 2009UrsTruly kotiNo ratings yet
- Rakesh Ali: Centre Manager (Edubridge Learning Pvt. LTD)Document2 pagesRakesh Ali: Centre Manager (Edubridge Learning Pvt. LTD)HRD CORP CONSULTANCYNo ratings yet