You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Yardi Commercial SuiteDocument52 pagesYardi Commercial SuiteSpicyNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Iritable Bowel SyndromeDocument30 pagesIritable Bowel SyndromeArnella HutagalungNo ratings yet
- MR15 Mechanical Engineering SyllabusDocument217 pagesMR15 Mechanical Engineering Syllabusramji_kkpNo ratings yet
- BWT Septron Line 31-61 Rev01!08!05-18 Opm enDocument56 pagesBWT Septron Line 31-61 Rev01!08!05-18 Opm enDavide Grioni100% (1)
- Publications FireSafetyDesign SDocument369 pagesPublications FireSafetyDesign SJayachandra Reddy AnnavaramNo ratings yet
- Congenital AnomaliesDocument69 pagesCongenital AnomaliesArnella HutagalungNo ratings yet
- Principles of Marketing Eighth Edition Philip Kotler and Gary ArmstrongDocument17 pagesPrinciples of Marketing Eighth Edition Philip Kotler and Gary ArmstrongJunaid KhalidNo ratings yet
- 2019 ASME Section V ChangesDocument61 pages2019 ASME Section V Changesmanisami7036100% (4)
- FIDIC delay and disruption standardsDocument7 pagesFIDIC delay and disruption standardsMohammad FayazNo ratings yet
- Siegfried Kracauer - Photography (1927)Document17 pagesSiegfried Kracauer - Photography (1927)Paul NadeauNo ratings yet
- SRS documentation of Virtual Classroom System , SRS documentation of Personal Identity Management ,SRS documentation of EMentoring for women system , SRS Documentation of Employee Performance Management SRS Documentation of Online TicketingDocument79 pagesSRS documentation of Virtual Classroom System , SRS documentation of Personal Identity Management ,SRS documentation of EMentoring for women system , SRS Documentation of Employee Performance Management SRS Documentation of Online Ticketingsaravanakumar1896% (26)
- Rcog PDFDocument14 pagesRcog PDFArnella HutagalungNo ratings yet
- Gitelman Syndrome Case Report Hypomagnesemia HypokalemiaDocument4 pagesGitelman Syndrome Case Report Hypomagnesemia HypokalemiaArnella HutagalungNo ratings yet
- ICP AnnalsofhepatologyDocument4 pagesICP AnnalsofhepatologyArnella HutagalungNo ratings yet
- Seminar Antenatal Conditions Intrahepatic Cholestasis of Pregnancy DR J MarlowDocument29 pagesSeminar Antenatal Conditions Intrahepatic Cholestasis of Pregnancy DR J MarlowArnella HutagalungNo ratings yet
- Cancer (Biokimia)Document20 pagesCancer (Biokimia)Arnella HutagalungNo ratings yet
- K - 34 Food Diversity (Gizi)Document28 pagesK - 34 Food Diversity (Gizi)Izaac JdevNo ratings yet
- Body Fluids Balance: Atan Baas SinuhajiDocument33 pagesBody Fluids Balance: Atan Baas SinuhajiArnella HutagalungNo ratings yet
- NEPHROLITHIASIS: Etiology, Composition, Management & PreventionDocument28 pagesNEPHROLITHIASIS: Etiology, Composition, Management & PreventionRuthra Devi NarayanasamyNo ratings yet
- ACGGuideline Liver Disease and Pregnancy 2016 PDFDocument19 pagesACGGuideline Liver Disease and Pregnancy 2016 PDFArnella HutagalungNo ratings yet
- Urinary Tract Infection: Infeksi Saluran KemihDocument35 pagesUrinary Tract Infection: Infeksi Saluran KemihArnella HutagalungNo ratings yet
- BHP K7 E-HealthDocument60 pagesBHP K7 E-HealthArnella HutagalungNo ratings yet
- Wellness Program (IKK)Document26 pagesWellness Program (IKK)Arnella HutagalungNo ratings yet
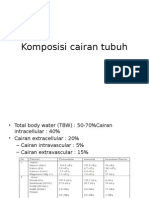
- Komposisi Cairan TubuhDocument2 pagesKomposisi Cairan TubuhArnella HutagalungNo ratings yet
- K6 BakulDocument36 pagesK6 BakulArnella HutagalungNo ratings yet
- MANAGEMENT OF TETANUS: CLINICAL FEATURES, DIAGNOSIS AND TREATMENTDocument7 pagesMANAGEMENT OF TETANUS: CLINICAL FEATURES, DIAGNOSIS AND TREATMENTArnella HutagalungNo ratings yet
- K - 21 Late Pregnancy Bleeding (Obgyn)Document45 pagesK - 21 Late Pregnancy Bleeding (Obgyn)Arnella HutagalungNo ratings yet
- Dep Kes Rentang UsiaDocument10 pagesDep Kes Rentang UsiaArnella HutagalungNo ratings yet
- Pathology of The AdnexaDocument59 pagesPathology of The AdnexaArnella HutagalungNo ratings yet
- GOLD Slideset 2014jan28Document119 pagesGOLD Slideset 2014jan28Arnella HutagalungNo ratings yet
- MANAGEMENT OF TETANUS: CLINICAL FEATURES, DIAGNOSIS AND TREATMENTDocument7 pagesMANAGEMENT OF TETANUS: CLINICAL FEATURES, DIAGNOSIS AND TREATMENTArnella HutagalungNo ratings yet
- J Neurol Neurosurg Psychiatry 2000 Farrar 292 301 Jurnal TetanusDocument11 pagesJ Neurol Neurosurg Psychiatry 2000 Farrar 292 301 Jurnal TetanusArnella HutagalungNo ratings yet
- Pathology of Gestational DiseasesDocument25 pagesPathology of Gestational DiseasesArnella HutagalungNo ratings yet
- Tetanus PDFDocument11 pagesTetanus PDFDwi Andriyani NimanNo ratings yet
- Pathology of The AdnexaDocument59 pagesPathology of The AdnexaArnella HutagalungNo ratings yet
- Mutaz Abdelrahim - Doa - MT-103Document17 pagesMutaz Abdelrahim - Doa - MT-103Minh KentNo ratings yet
- Case Study - Help DocumentDocument2 pagesCase Study - Help DocumentRahNo ratings yet
- 2 Case StudyDocument8 pages2 Case Studysehrish khawerNo ratings yet
- Module 2 What It Means To Be AI FirstDocument85 pagesModule 2 What It Means To Be AI FirstSantiago Ariel Bustos YagueNo ratings yet
- Research of William Wells at HarvardDocument10 pagesResearch of William Wells at HarvardARGHA MANNANo ratings yet
- 8086 Microprocessor: J Srinivasa Rao Govt Polytechnic Kothagudem KhammamDocument129 pages8086 Microprocessor: J Srinivasa Rao Govt Polytechnic Kothagudem KhammamAnonymous J32rzNf6ONo ratings yet
- Foundry Technology GuideDocument34 pagesFoundry Technology GuidePranav Pandey100% (1)
- Costos estándar clase viernesDocument9 pagesCostos estándar clase viernesSergio Yamil Cuevas CruzNo ratings yet
- What Is Chemical EngineeringDocument4 pagesWhat Is Chemical EngineeringgersonNo ratings yet
- 2020 - Audcap1 - 2.3 RCCM - BunagDocument1 page2020 - Audcap1 - 2.3 RCCM - BunagSherilyn BunagNo ratings yet
- MMH Dan StoringDocument13 pagesMMH Dan Storingfilza100% (1)
- Offshore Wind Turbine 6mw Robust Simple EfficientDocument4 pagesOffshore Wind Turbine 6mw Robust Simple EfficientCristian Jhair PerezNo ratings yet
- Edexcel A2 Biology 6BI06Document7 pagesEdexcel A2 Biology 6BI06abhayNo ratings yet
- Yamaha RX-A3000 - V3067Document197 pagesYamaha RX-A3000 - V3067jaysonNo ratings yet
- Online Music QuizDocument3 pagesOnline Music QuizGiang VõNo ratings yet
- Lks Bahasa Inggris Kelas Vii Semester 1 Dan 2Document6 pagesLks Bahasa Inggris Kelas Vii Semester 1 Dan 2ꓰꓡꓡꓰꓠ.ꓓꓰꓖꓰꓠꓰꓣꓰꓢꓢ.No ratings yet
- Module 7 - Assessment of Learning 1 CoursepackDocument7 pagesModule 7 - Assessment of Learning 1 CoursepackZel FerrelNo ratings yet
- 26th April 2021 ES Submission - CloudKitchens - ProfessorSriramDocument16 pages26th April 2021 ES Submission - CloudKitchens - ProfessorSriramSamarth LahotiNo ratings yet
- Irc SP 65-2005 PDFDocument32 pagesIrc SP 65-2005 PDFAjay Kumar JainNo ratings yet
- 01 WELD-2022 Ebrochure 3Document5 pages01 WELD-2022 Ebrochure 3Arpita patelNo ratings yet
- Primary Homework Help Food ChainsDocument7 pagesPrimary Homework Help Food Chainsafnaxdxtloexll100% (1)