You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 2019 Auto Truck Key Blank Reference PDFDocument188 pages2019 Auto Truck Key Blank Reference PDFAlbert RodaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- School Form 8 Grade 3Document20 pagesSchool Form 8 Grade 3Mimi Ng PinasNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- RL78 L1B UsermanualDocument1,062 pagesRL78 L1B UsermanualHANUMANTHA RAO GORAKANo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Angles, Bearings and AzimuthDocument10 pagesAngles, Bearings and AzimuthMarc Dared CagaoanNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Aloe Vera An Ancient Herb For Modern Dentistry-A LDocument7 pagesAloe Vera An Ancient Herb For Modern Dentistry-A LRuth Ransel Yadao ValentinNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Adolescence Problems PPT 1Document25 pagesAdolescence Problems PPT 1akhila appukuttanNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Symmetrir and Order. Reasons To Live According The LodgeDocument6 pagesSymmetrir and Order. Reasons To Live According The LodgeAnonymous zfNrN9NdNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Annexure To SOW 3 STD Specification For Welding and NDT PipingDocument15 pagesAnnexure To SOW 3 STD Specification For Welding and NDT PipingASHISH GORDENo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- MATLAB For Data VisualizationDocument63 pagesMATLAB For Data Visualizationfahmi fawjiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Crop Science SyllabusDocument42 pagesCrop Science Syllabusbetty makushaNo ratings yet
- Army Public School No.1 Jabalpur Practical List - Computer Science Class - XIIDocument4 pagesArmy Public School No.1 Jabalpur Practical List - Computer Science Class - XIIAdityaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- GRADE 302: Element Content (%)Document3 pagesGRADE 302: Element Content (%)Shashank Saxena100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Guide To Funeral Ceremonies and PrayersDocument26 pagesA Guide To Funeral Ceremonies and PrayersJohn DoeNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On The Margins - A Study of The Experiences of Transgender College StudentsDocument14 pagesOn The Margins - A Study of The Experiences of Transgender College StudentsRory J. BlankNo ratings yet
- Decolonization DBQDocument3 pagesDecolonization DBQapi-493862773No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CD4 12-P374493Document30 pagesCD4 12-P374493suraj_savant1No ratings yet
- Business Mathematics (Matrix)Document3 pagesBusiness Mathematics (Matrix)MD HABIBNo ratings yet
- Annual Report 2022 2Document48 pagesAnnual Report 2022 2Dejan ReljinNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- PCZ 1503020 CeDocument73 pagesPCZ 1503020 Cedanielradu27No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Important Instructions For Winter-2020 MCQ Based Online ExaminationDocument1 pageImportant Instructions For Winter-2020 MCQ Based Online Examinationdenoh32751No ratings yet
- Assignment OSDocument11 pagesAssignment OSJunaidArshadNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Code of Conduct For Public OfficialDocument17 pagesCode of Conduct For Public OfficialHaNo ratings yet
- Family Planning MethodsDocument20 pagesFamily Planning MethodsRoel Marcial100% (2)
- Job Stress InterventionsDocument5 pagesJob Stress InterventionscocaralucamihaelaNo ratings yet
- Competent Testing Requirements As Per Factory ActDocument3 pagesCompetent Testing Requirements As Per Factory Actamit_lunia100% (1)
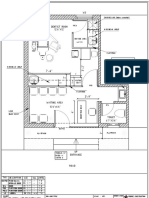
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- LC 67002000 B Hr-Jumbo enDocument2 pagesLC 67002000 B Hr-Jumbo enJulio OrtegaNo ratings yet
- Benson Ivor - The Zionist FactorDocument234 pagesBenson Ivor - The Zionist Factorblago simeonov100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Solving Systems of Linear Equations in Three Variables: You Should LearnDocument8 pagesSolving Systems of Linear Equations in Three Variables: You Should LearnTheodore JoaquinnNo ratings yet
- Design of Ka-Band Low Noise Amplifier Using CMOS TechnologyDocument6 pagesDesign of Ka-Band Low Noise Amplifier Using CMOS TechnologyEditor IJRITCCNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)