You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Biopsychosocial Formulation Manual A Guide For Mental Health Professionals PDFDocument178 pagesThe Biopsychosocial Formulation Manual A Guide For Mental Health Professionals PDFLeidy Yiseth Cárdenas100% (4)
- The Galeniko-Noone MethodDocument82 pagesThe Galeniko-Noone MethodLouFerrignoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Post TestDocument9 pagesPost TestPradnya Paramitha100% (2)
- Part C Volume VI General Medicine I NEET PG 21 06Document18 pagesPart C Volume VI General Medicine I NEET PG 21 06C Bala DiwakeshNo ratings yet
- Rheumatology 05Document6 pagesRheumatology 05C Bala DiwakeshNo ratings yet
- How Rich Countries Became Rich and Why Poor Countries Remain Poor: It's The Economic Structure - . - Duh!Document55 pagesHow Rich Countries Became Rich and Why Poor Countries Remain Poor: It's The Economic Structure - . - Duh!C Bala DiwakeshNo ratings yet
- Elevation of Serum Creatinine Phosphokinase Level As A Marker For Severity in Acute OrganophosphorouDocument18 pagesElevation of Serum Creatinine Phosphokinase Level As A Marker For Severity in Acute OrganophosphorouC Bala DiwakeshNo ratings yet
- Second Seat Allotment List MBBS - College - List - Phase2Document94 pagesSecond Seat Allotment List MBBS - College - List - Phase2C Bala DiwakeshNo ratings yet
- CrownsDocument6 pagesCrownsC Bala DiwakeshNo ratings yet
- Nutrition in Renal DiseasesDocument14 pagesNutrition in Renal DiseasesC Bala DiwakeshNo ratings yet
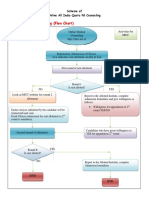
- Flow Chart of Online Counseling PDFDocument2 pagesFlow Chart of Online Counseling PDFAnonymous 4gnjzsNo ratings yet
- For All India Quota/ Deemed/ Central Universities Online Counseling For Post-Graduate Medical/ Dental /diploma SeatsDocument15 pagesFor All India Quota/ Deemed/ Central Universities Online Counseling For Post-Graduate Medical/ Dental /diploma SeatsC Bala DiwakeshNo ratings yet
- Cms 2017 Obc AnnexureDocument4 pagesCms 2017 Obc AnnexureC Bala DiwakeshNo ratings yet
- PG Counseling Scheme 17Document13 pagesPG Counseling Scheme 17Rohit BansalNo ratings yet
- DNB (Post MBBS) Indicative Seat Matrix Jan 2018 - 03.05.2018 PDFDocument140 pagesDNB (Post MBBS) Indicative Seat Matrix Jan 2018 - 03.05.2018 PDFSahid KapoorNo ratings yet
- MD R1Document555 pagesMD R1kashif zafarNo ratings yet
- GeneticsDocument5 pagesGeneticsC Bala DiwakeshNo ratings yet
- DNB (Post Diploma) Emergency Medicine Indicative Seat Matrix Jan 2015Document3 pagesDNB (Post Diploma) Emergency Medicine Indicative Seat Matrix Jan 2015C Bala DiwakeshNo ratings yet
- MD MS Prospectus July 2017 Session UpdatedDocument40 pagesMD MS Prospectus July 2017 Session UpdatedC Bala DiwakeshNo ratings yet
- Instructions For Eapar in SparrowDocument4 pagesInstructions For Eapar in SparrowC Bala DiwakeshNo ratings yet
- Biology XII SET-A - Cbse GuessDocument8 pagesBiology XII SET-A - Cbse GuessC Bala DiwakeshNo ratings yet
- PG Revised Cut OffDocument2 pagesPG Revised Cut OffC Bala DiwakeshNo ratings yet
- Recombinant Dna TechnologyDocument5 pagesRecombinant Dna TechnologyC Bala DiwakeshNo ratings yet
- Biology Midterm ExamDocument19 pagesBiology Midterm ExamC Bala DiwakeshNo ratings yet
- Prokaryotes and EukaryotesDocument6 pagesProkaryotes and EukaryotesC Bala DiwakeshNo ratings yet
- Azetecs EmpireDocument7 pagesAzetecs EmpireC Bala DiwakeshNo ratings yet
- Fractal Time PDFDocument64 pagesFractal Time PDFSrdjan DrazovicNo ratings yet
- DNB Cet June 2018Document3 pagesDNB Cet June 2018C Bala DiwakeshNo ratings yet
- Marking System 12th Biology Sample Paper 1 PDFDocument26 pagesMarking System 12th Biology Sample Paper 1 PDFC Bala DiwakeshNo ratings yet
- The Spontaneous Healing of Belief: Audio SummaryDocument1 pageThe Spontaneous Healing of Belief: Audio SummaryC Bala DiwakeshNo ratings yet
- UserManual ApplicationForm v1.2Document5 pagesUserManual ApplicationForm v1.2C Bala DiwakeshNo ratings yet
- Image InstructionsDocument2 pagesImage InstructionsC Bala DiwakeshNo ratings yet
- Drug Study - CaDocument3 pagesDrug Study - Casaint_ronald8No ratings yet
- Cardiac Enzymes - KulDocument39 pagesCardiac Enzymes - KulAnonymous J1iWk2xNo ratings yet
- Guía de Diabetes y PsicosisDocument5 pagesGuía de Diabetes y PsicosiskarlunchoNo ratings yet
- Benefit 1Document10 pagesBenefit 1HL LauNo ratings yet
- Myotonic DiseaseDocument11 pagesMyotonic DiseaseOhlee TanNo ratings yet
- Deborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDocument5 pagesDeborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDago Angel Prieto PalavecinoNo ratings yet
- Dyspnea Orthopnea PND PDFDocument3 pagesDyspnea Orthopnea PND PDFNurulAlviFauzianaNo ratings yet
- Precision Business Insights (PBI) : We Provide Answers To Your Questions and Deliver Actionable InsightsDocument12 pagesPrecision Business Insights (PBI) : We Provide Answers To Your Questions and Deliver Actionable InsightsSai KrishnaNo ratings yet
- Sexual AbuseDocument2 pagesSexual AbuseRuth AngelaNo ratings yet
- AFCC Powerpoint 2017 Pruter Powerpoint CC DR ChildressDocument8 pagesAFCC Powerpoint 2017 Pruter Powerpoint CC DR Childressa.petersritNo ratings yet
- Nursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation EvaluationDocument4 pagesNursing Care Plan For Mother:: Sno Assessment Diagnosis Planning Implementation Evaluationmishti100% (1)
- Amoxicillin and Clavula NateDocument4 pagesAmoxicillin and Clavula NateRoberto BenziNo ratings yet
- Angiotensin II Receptor Blockers-PowerpointDocument16 pagesAngiotensin II Receptor Blockers-PowerpointRoxanne Postrano De VeraNo ratings yet
- Oral Chondroprotective Agents - Part IIDocument5 pagesOral Chondroprotective Agents - Part IItaner_soysurenNo ratings yet
- Prescription & Its PartsDocument8 pagesPrescription & Its Partsmadhumay23100% (1)
- ZDocument3 pagesZBenjamin TantiansuNo ratings yet
- ADHD Guidance-September 2013Document6 pagesADHD Guidance-September 2013Claude JousselinNo ratings yet
- CSA11 CholelithiasisDocument3 pagesCSA11 CholelithiasisBerlon LacsonNo ratings yet
- SML IsuzuDocument10 pagesSML IsuzuPankajNo ratings yet
- Psychiatric Nursing ChecklistDocument4 pagesPsychiatric Nursing ChecklistNevea CariñoNo ratings yet
- Paternal Postnatal Psychiatric - IllnessesDocument202 pagesPaternal Postnatal Psychiatric - IllnessesBalasubrahmanya K. R.No ratings yet
- College of Nursing: Cebu Normal UniversityDocument5 pagesCollege of Nursing: Cebu Normal UniversityChelsea WuNo ratings yet
- FitoterapiDocument8 pagesFitoterapiNetta JaneNo ratings yet
- Hps Health - Indian Sanskrit Damar Tantra Sutra (Part 5), Urine TherapyDocument4 pagesHps Health - Indian Sanskrit Damar Tantra Sutra (Part 5), Urine TherapyAashishh PatilNo ratings yet
- Serous Fluids AnalysisDocument15 pagesSerous Fluids AnalysisMustafa Khandgawi100% (1)
- Assessment of Development and GrowthDocument21 pagesAssessment of Development and Growthdrng48No ratings yet
- Evaluation of Intraoral Verticosagittal Hashemi2008Document4 pagesEvaluation of Intraoral Verticosagittal Hashemi2008carolina vega hernandezNo ratings yet