You might also like
- AOMSI Calender of Events 2024 FinalDocument4 pagesAOMSI Calender of Events 2024 Finalsevattapillai100% (1)
- Sterilization and AsepsisDocument48 pagesSterilization and AsepsissevattapillaiNo ratings yet
- SBV Dissertation Template 2017Document22 pagesSBV Dissertation Template 2017sevattapillaiNo ratings yet
- Best Practices OMFS DEPTDocument2 pagesBest Practices OMFS DEPTsevattapillaiNo ratings yet
- Antibiotics in Oral & Maxillofacial SurgeryDocument50 pagesAntibiotics in Oral & Maxillofacial SurgerysevattapillaiNo ratings yet
- Jackie ChanDocument1 pageJackie ChansevattapillaiNo ratings yet
- Life of Gajanan Vijay Granthi UneditedDocument63 pagesLife of Gajanan Vijay Granthi UneditedsevattapillaiNo ratings yet
- Life and Work of Shri Hans Ji MaharajDocument75 pagesLife and Work of Shri Hans Ji Maharajsevattapillai100% (1)
- Oral LymphangiomaDocument8 pagesOral LymphangiomasevattapillaiNo ratings yet
- CANINE Impaction Oral SurgeryDocument46 pagesCANINE Impaction Oral SurgeryFourthMolar.com100% (5)
- HSR ParentDocument9 pagesHSR ParentsevattapillaiNo ratings yet
- Life of Gopalbua Kelkar MaharajDocument1 pageLife of Gopalbua Kelkar MaharajsevattapillaiNo ratings yet
- Flap Design For Minor Oral SurgeryDocument22 pagesFlap Design For Minor Oral SurgerysevattapillaiNo ratings yet
- Sri Vidya Upasakas - Bhaskara Prakasha AshramDocument7 pagesSri Vidya Upasakas - Bhaskara Prakasha Ashramsevattapillai75% (4)
- Life of Swamisut MaharajDocument2 pagesLife of Swamisut MaharajsevattapillaiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
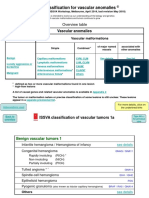
- ISSVA Classification 2018 PDFDocument20 pagesISSVA Classification 2018 PDFIgor YonekuraNo ratings yet
- Issva Classification 2014 Final TrialDocument20 pagesIssva Classification 2014 Final TrialFrancis MunguíaNo ratings yet
- Vascular Anomalies PresentationDocument45 pagesVascular Anomalies PresentationMhinory OctNo ratings yet
- Blood Vessel PathologyDocument99 pagesBlood Vessel PathologyGeorge Hanania100% (1)
- Blue Red LesionDocument14 pagesBlue Red LesionXara Barretto MagadiaNo ratings yet
- EASL-GL Benign Tumor LiverDocument13 pagesEASL-GL Benign Tumor LiveroliviaNo ratings yet
- Healthmedicinet Com II 2014 JanDocument326 pagesHealthmedicinet Com II 2014 JanHeal ThmedicinetNo ratings yet
- Journal Diagnosis and Management of A Tympanic Membrane HemangiomaDocument9 pagesJournal Diagnosis and Management of A Tympanic Membrane HemangiomaAndriyani YaniNo ratings yet
- Matary Clinical - 2013 (WWW - Afriqa Sat - Com)Document338 pagesMatary Clinical - 2013 (WWW - Afriqa Sat - Com)Ahmed Attia100% (1)
- Pediatric DermatologyDocument47 pagesPediatric DermatologyAmr Abualrub100% (2)
- Lasers Laser Like 2 PDFDocument14 pagesLasers Laser Like 2 PDFRidha Ramadina WidiatmaNo ratings yet
- Treatment of Infantile Capillary Hemangioma of The Eyelid With Systemic PropranololDocument32 pagesTreatment of Infantile Capillary Hemangioma of The Eyelid With Systemic PropranololMargaretha Syane LientunganNo ratings yet
- Birthmarks Identificationandmx201205ryanDocument4 pagesBirthmarks Identificationandmx201205ryanDanielcc LeeNo ratings yet
- Immediate Care of The NewbornDocument11 pagesImmediate Care of The NewbornHannahKarizaNo ratings yet
- Blood Vessels QuizDocument28 pagesBlood Vessels Quiztatti999No ratings yet
- Newborns Undergo Profound Physiologic Changes at The Moment of BirthDocument8 pagesNewborns Undergo Profound Physiologic Changes at The Moment of BirthUri ELNo ratings yet
- GentleLASE Treatment GuidelinesDocument7 pagesGentleLASE Treatment Guidelinessoma_ah100% (7)
- Pediatric OtolaryngologyDocument242 pagesPediatric OtolaryngologyDrMohmd ZidaanNo ratings yet
- Connective Tissue TumorsDocument60 pagesConnective Tissue TumorsRahul Nagda67% (3)
- Hemangioma PresentationDocument18 pagesHemangioma Presentationplastic guardiansNo ratings yet
- EyelidsDocument96 pagesEyelidsArwa QishtaNo ratings yet
- Pediatric Dermatology MCQsDocument53 pagesPediatric Dermatology MCQsDr.Tawheed89% (18)
- Skin Nail HairDocument48 pagesSkin Nail HairkitsilcNo ratings yet
- Benign Tumors of LarynxDocument48 pagesBenign Tumors of LarynxVilZan MominNo ratings yet
- Benign Liver Tumors: HemangiomaDocument6 pagesBenign Liver Tumors: HemangiomaEnricoSetiawanNo ratings yet
- Pathology of Blood VesselsDocument80 pagesPathology of Blood VesselsiqiqiqiqiqNo ratings yet
- Eponyms SyndromesDocument23 pagesEponyms Syndromestekennn021No ratings yet
- Curriculum Vitae Werner EnglDocument13 pagesCurriculum Vitae Werner EngldiarioepocaNo ratings yet
- 63 - CASE REPORT Epulis GranulomaDocument3 pages63 - CASE REPORT Epulis GranulomaRina NovitrianiNo ratings yet
- 9 Mesenchymal Tumors 2Document77 pages9 Mesenchymal Tumors 2Ther Ray100% (1)