You might also like
- 13 14 1 PB PDFDocument7 pages13 14 1 PB PDFKomang Tri Adi SuparwatiNo ratings yet
- Wound Healing LectureDocument80 pagesWound Healing LecturegogmasiraitNo ratings yet
- Standardized Balance Tests for Fall Risk AssessmentDocument8 pagesStandardized Balance Tests for Fall Risk AssessmentAlvin OngNo ratings yet
- PrinciplesWoundHealing WCCSpring2011 PDFDocument5 pagesPrinciplesWoundHealing WCCSpring2011 PDFaajelNo ratings yet
- Wound Healing LectureDocument80 pagesWound Healing LecturegogmasiraitNo ratings yet
- Wound Healing Basic Concepts BhavsarDocument47 pagesWound Healing Basic Concepts BhavsarKomang Tri Adi SuparwatiNo ratings yet
- Journal of International Medical Research 2009 Velnar 1528 42Document15 pagesJournal of International Medical Research 2009 Velnar 1528 42NoorliyyantiNo ratings yet
- Neurological PhysiotherapyDocument252 pagesNeurological PhysiotherapyZrakaSunca93% (14)
- Temporamandibula JointDocument22 pagesTemporamandibula JointKomang Tri Adi SuparwatiNo ratings yet
- Mandibular Movements Up L of DDocument79 pagesMandibular Movements Up L of DkrondanNo ratings yet
- Neurological PhysiotherapyDocument252 pagesNeurological PhysiotherapyZrakaSunca93% (14)
- TMJ DisordersDocument20 pagesTMJ DisordersErisa BllakajNo ratings yet
- Temporamandibula JointDocument22 pagesTemporamandibula JointKomang Tri Adi SuparwatiNo ratings yet
- Temporamandibula JointDocument22 pagesTemporamandibula JointKomang Tri Adi SuparwatiNo ratings yet
- Joint Pain Leaflet PDFDocument12 pagesJoint Pain Leaflet PDFSuaeni Kurnia Wirda100% (1)
- Si PDFDocument7 pagesSi PDFKomang Tri Adi SuparwatiNo ratings yet
- Temporamandibula JointDocument22 pagesTemporamandibula JointKomang Tri Adi SuparwatiNo ratings yet
- Doping and Performance Enhancing Drug Use in SportDocument5 pagesDoping and Performance Enhancing Drug Use in SportKomang Tri Adi SuparwatiNo ratings yet
- Saraf PeriferDocument41 pagesSaraf PeriferLaurensia Erlina NataliaNo ratings yet
- CN - Jurnal Lansia 1Document5 pagesCN - Jurnal Lansia 1vidiaherdinaNo ratings yet
- CN - Jurnal Lansia 1Document5 pagesCN - Jurnal Lansia 1vidiaherdinaNo ratings yet
- Head & Neck - Deep Cervical Fascia &cervical PlexusDocument9 pagesHead & Neck - Deep Cervical Fascia &cervical PlexusKomang Tri Adi SuparwatiNo ratings yet
- Ems UnitDocument28 pagesEms UnitKomang Tri Adi SuparwatiNo ratings yet
- Bdi Tdi PDFDocument52 pagesBdi Tdi PDFKomang Tri Adi SuparwatiNo ratings yet
- Indonesian WhoqolDocument5 pagesIndonesian WhoqolSri Nindita RuslanNo ratings yet
- LaserDocument23 pagesLaserKomang Tri Adi SuparwatiNo ratings yet
- Icf CyDocument351 pagesIcf CyDyandraFA100% (1)
- Regeneration. Wound Healing: October 10, 2006Document47 pagesRegeneration. Wound Healing: October 10, 2006Komang Tri Adi SuparwatiNo ratings yet
- Head & Neck - Deep Cervical Fascia &cervical PlexusDocument9 pagesHead & Neck - Deep Cervical Fascia &cervical PlexusKomang Tri Adi SuparwatiNo ratings yet
- Wound Healing LectureDocument80 pagesWound Healing LecturegogmasiraitNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- AudiDocument21 pagesAudiapi-281175594No ratings yet
- Unit 3 Basic TestDocument2 pagesUnit 3 Basic TestksawerystrukNo ratings yet
- Encyclopaedia of Chess OpeningsDocument4 pagesEncyclopaedia of Chess OpeningsAdi Susanto56% (9)
- Correlated Subqueries: Mona KhalilDocument40 pagesCorrelated Subqueries: Mona Khalilanubhav582No ratings yet
- Vac Truck Insp ChecklistDocument4 pagesVac Truck Insp ChecklistMladi AktivniNo ratings yet
- Horses in Europe: by Carolina LiljenstolpeDocument32 pagesHorses in Europe: by Carolina LiljenstolpeMilos StojanovicNo ratings yet
- MSK Us ProtocolsDocument40 pagesMSK Us Protocolsjamir59No ratings yet
- Dashing Product Manual 38x18cmDocument8 pagesDashing Product Manual 38x18cmalberto celiNo ratings yet
- Member LedgersDocument205 pagesMember LedgersDhruv ChandwaniNo ratings yet
- 03 Preparation Items PDFDocument90 pages03 Preparation Items PDFTecnoCar Services SDRNo ratings yet
- 303 ProjectDocument4 pages303 ProjectChristian SawayaNo ratings yet
- Er Est Tter Ttest R ST Ier Iest: (Than)Document3 pagesEr Est Tter Ttest R ST Ier Iest: (Than)Barbara NevesNo ratings yet
- Mayhem Entry 2015Document1 pageMayhem Entry 2015thedietdocNo ratings yet
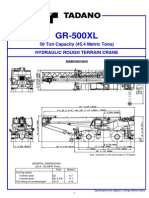
- Specifikasi Tadano GR-500XLDocument11 pagesSpecifikasi Tadano GR-500XLHaka Surya GratamaNo ratings yet
- Star FallDocument51 pagesStar FallАлиса ШмароваNo ratings yet
- Projectile Motion (Worksheet)Document6 pagesProjectile Motion (Worksheet)Hassan AideedNo ratings yet
- My BetsDocument1 pageMy BetsAbuo IgboanugwoNo ratings yet
- Unofficial FAQ and Clarifications Based On The French Edition of King of TokyoDocument2 pagesUnofficial FAQ and Clarifications Based On The French Edition of King of TokyoOlga G. CabezasNo ratings yet
- FSF Series fsf350 fsf450 6w Ss Pump Usual Manual EnglishDocument2 pagesFSF Series fsf350 fsf450 6w Ss Pump Usual Manual EnglishEva Dewi PuspitaNo ratings yet
- Oven PengeringDocument32 pagesOven PengeringDwikiNo ratings yet
- Cheerdance Competition: A. EligibilityDocument2 pagesCheerdance Competition: A. EligibilityPianista KoNo ratings yet
- Betting Data 2020 21 - Ver 7.0Document192 pagesBetting Data 2020 21 - Ver 7.0Kaung MyatNo ratings yet
- Bangladesh Spinning Mills (BTMA)Document21 pagesBangladesh Spinning Mills (BTMA)Siddique Ahmed80% (10)
- 5 ĐỀ THI HK 1 - Tiếng Anh 3 Global có đáp ánDocument18 pages5 ĐỀ THI HK 1 - Tiếng Anh 3 Global có đáp ánNhàn BeeNo ratings yet
- OthersDocument15 pagesOthersAlfie b. bagsaoNo ratings yet
- Elektronski RelejiDocument11 pagesElektronski RelejiElharun Karic0% (1)
- eMRCS AnatomyDocument158 pageseMRCS AnatomyNayem Hossain Hemu50% (2)
- Pinoy TambayanDocument33 pagesPinoy TambayanPinoy TvNo ratings yet
- Case Presentation - Closed Fracture Radius Ulna PediatricDocument30 pagesCase Presentation - Closed Fracture Radius Ulna PediatriciamboredtiredNo ratings yet
- This Is My WorldDocument3 pagesThis Is My Worldmadeinengland2No ratings yet