You might also like
- (Jian-Gang Shi, Wen Yuan, Jing-Chuan Sun (Eds.) ) A (B-Ok - CC)Document305 pages(Jian-Gang Shi, Wen Yuan, Jing-Chuan Sun (Eds.) ) A (B-Ok - CC)Lorena BurdujocNo ratings yet
- 2019 Neurosurgery by Example - Spinal NeurosurgeryDocument281 pages2019 Neurosurgery by Example - Spinal NeurosurgeryPermata GBKP Runggun SurabayaNo ratings yet
- Co-Existence of Carcinoma Tongue With Pulmonary TuberculosisDocument2 pagesCo-Existence of Carcinoma Tongue With Pulmonary TuberculosisAnnastasia MiaNo ratings yet
- Curriculum Vitae: Personal InformationDocument3 pagesCurriculum Vitae: Personal InformationAnnastasia MiaNo ratings yet
- Oral Manifestations in Pulmonary Diseases - Too Often A Neglected ProblemDocument7 pagesOral Manifestations in Pulmonary Diseases - Too Often A Neglected ProblemAnnastasia MiaNo ratings yet
- Obat 2 AnDocument8 pagesObat 2 AnFirda Muthia ElsyantyNo ratings yet
- Irritant Contact Dermatitis Mechanisms To Repair 2155 9554.1000246Document8 pagesIrritant Contact Dermatitis Mechanisms To Repair 2155 9554.1000246Annastasia MiaNo ratings yet
- JadwalDocument1 pageJadwalAnnastasia MiaNo ratings yet
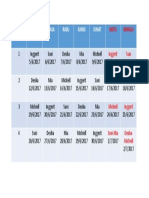
- Weekly Schedule for Inggerit, Suni, Desika, Mia and MichiellDocument1 pageWeekly Schedule for Inggerit, Suni, Desika, Mia and MichiellAnnastasia MiaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Business Communication - Case - Josh Miller Is A Finance Student - 2Document4 pagesBusiness Communication - Case - Josh Miller Is A Finance Student - 2Sailpoint CourseNo ratings yet
- A Review of The Book That Made Your World. by Vishal MangalwadiDocument6 pagesA Review of The Book That Made Your World. by Vishal Mangalwadigaylerob100% (1)
- SkipTheFlip Physical PDFDocument230 pagesSkipTheFlip Physical PDFSebi100% (4)
- Philo 12Document2 pagesPhilo 12Rachel LaganNo ratings yet
- 2004 Swamee, Prabhata K. Rathie, Pushpa N. - Exact Solutions For Normal Depth ProblemDocument9 pages2004 Swamee, Prabhata K. Rathie, Pushpa N. - Exact Solutions For Normal Depth Problemjosue.angelo9459No ratings yet
- Syllabus Mac1105 M 530 - 8 PM 203080Document6 pagesSyllabus Mac1105 M 530 - 8 PM 203080api-261843361No ratings yet
- Letters and Treaties by Mohammad PBUH-3 PDFDocument19 pagesLetters and Treaties by Mohammad PBUH-3 PDFAbdulaziz Khattak Abu FatimaNo ratings yet
- Types of Errors and Coding TechniquesDocument11 pagesTypes of Errors and Coding TechniquesTiffany KagsNo ratings yet
- Motion For Reconsideration (Bolado & Aranilla)Document4 pagesMotion For Reconsideration (Bolado & Aranilla)edrynejethNo ratings yet
- Genealogy On June 09-2003Document25 pagesGenealogy On June 09-2003syedyusufsam92100% (3)
- Civet CoffeeDocument8 pagesCivet CoffeeAn NhiênNo ratings yet
- Permissions Problems - DeniedDocument5 pagesPermissions Problems - DeniedGeo KalNo ratings yet
- Fluid Flow and Kinetics Adam PowellDocument26 pagesFluid Flow and Kinetics Adam PowellSanki KurliNo ratings yet
- Prambanan Temple LegendDocument1 pagePrambanan Temple LegendClara NadaNo ratings yet
- Personal Narrative EssayDocument3 pagesPersonal Narrative Essayapi-510316103No ratings yet
- Pulp Fiction DeconstructionDocument3 pagesPulp Fiction Deconstructiondomatthews09No ratings yet
- Computers in Human Behavior: Aideen Lawlor, DR Jurek KirakowskiDocument11 pagesComputers in Human Behavior: Aideen Lawlor, DR Jurek KirakowskiAlejandro BejaranoNo ratings yet
- Objective/Multiple Type QuestionDocument14 pagesObjective/Multiple Type QuestionMITALI TAKIAR100% (1)
- Microcontrollers vs MicroprocessorsDocument90 pagesMicrocontrollers vs MicroprocessorsMehmet AşıkNo ratings yet
- Anthony Browder - The Mysteries of MelaninDocument4 pagesAnthony Browder - The Mysteries of MelaninHidden Truth82% (11)
- Department of Information TechnologyDocument1 pageDepartment of Information TechnologyMuhammad ZeerakNo ratings yet
- PH.D Scholars List 01022016Document64 pagesPH.D Scholars List 01022016vishalNo ratings yet
- 5 Job Interview Tips For IntrovertsDocument5 pages5 Job Interview Tips For IntrovertsSendhil RevuluriNo ratings yet
- Central Venous Access Devices (Cvads) andDocument68 pagesCentral Venous Access Devices (Cvads) andFitri ShabrinaNo ratings yet
- Timeline of The Human SocietyDocument3 pagesTimeline of The Human SocietyAtencio Barandino JhonilNo ratings yet
- Rietveld Made Easy - OverviewDocument3 pagesRietveld Made Easy - Overviewhp2020No ratings yet
- Computerised Accounting SystemDocument14 pagesComputerised Accounting SystemramneekdadwalNo ratings yet
- Hamlet Act 3 Scene 1Document4 pagesHamlet Act 3 Scene 1Αθηνουλα ΑθηναNo ratings yet
- Winning Market Through Market Oriented Strategic PlanningDocument25 pagesWinning Market Through Market Oriented Strategic PlanningKafi Mahmood NahinNo ratings yet
- Temenoff BiomaterialsDocument0 pagesTemenoff BiomaterialsJason Chou0% (9)