You might also like
- CholeraDocument5 pagesCholerabishnu011978No ratings yet
- Nephrotic SyndromeDocument43 pagesNephrotic SyndromegopscharanNo ratings yet
- Acute Lymphoblastic LeukemiaDocument25 pagesAcute Lymphoblastic Leukemiaapi-396564080No ratings yet
- Anaphylaxis Reaction & Drug Allergy 2Document47 pagesAnaphylaxis Reaction & Drug Allergy 2telusurNo ratings yet
- 1506359236-Assignment 13 - Diagnosing Schizophrenia and Other Psychotic DisordersDocument4 pages1506359236-Assignment 13 - Diagnosing Schizophrenia and Other Psychotic DisordersRita Prince0% (1)
- Insulin ShockDocument9 pagesInsulin ShockMarina CiburciuNo ratings yet
- History of Old ClientDocument33 pagesHistory of Old ClientMuhammad Aamir100% (1)
- Introduction Diabetic MellitusDocument3 pagesIntroduction Diabetic MellitusharpreetsainiNo ratings yet
- Carbon Monoxide Poisoning in ChildrenDocument10 pagesCarbon Monoxide Poisoning in ChildrenSubash PaudealNo ratings yet
- Nurs 641 Case Study PresentationDocument12 pagesNurs 641 Case Study Presentationapi-251235373No ratings yet
- Clinical Features of Renal DiseaseDocument80 pagesClinical Features of Renal DiseaseIdiAmadouNo ratings yet
- Cerebral Malaria (CM) Prof. WBP Matuja, MuhasDocument20 pagesCerebral Malaria (CM) Prof. WBP Matuja, MuhasAnonymous TCZf45C10No ratings yet
- (1479683X - European Journal of Endocrinology) Geographic Variations in The Frequency of Thyroid Disorders and Thyroid Peroxidase Antibodies in Persons Without Former Thyroid Disease Within GermanyDocument9 pages(1479683X - European Journal of Endocrinology) Geographic Variations in The Frequency of Thyroid Disorders and Thyroid Peroxidase Antibodies in Persons Without Former Thyroid Disease Within GermanyArul ThiyagarajanNo ratings yet
- Hepatocellular Carcinoma: Dr. Isbandiyah, SPPDDocument26 pagesHepatocellular Carcinoma: Dr. Isbandiyah, SPPDMeta ShofiaNo ratings yet
- Intra - Abdominal HypertensionDocument40 pagesIntra - Abdominal HypertensionBayu Surya Dana100% (1)
- Bleeding & WoundsDocument28 pagesBleeding & WoundsSemo SupraNo ratings yet
- Anxiety and Stress-Related DisordersDocument26 pagesAnxiety and Stress-Related Disordersunpredictable_stoneNo ratings yet
- Printed Material Module 7 Gastrointestinal System Drugs - PDFDocument45 pagesPrinted Material Module 7 Gastrointestinal System Drugs - PDFShang MacarayonNo ratings yet
- AUTOIMMUNEDocument75 pagesAUTOIMMUNEEva Boje-JugadorNo ratings yet
- Peculiarities of Pediatric Surgical PatientDocument19 pagesPeculiarities of Pediatric Surgical PatientAhmad Abu KushNo ratings yet
- Rheumatoid ArthritisDocument14 pagesRheumatoid ArthritisLorebell100% (5)
- Hirschprung DiseaseDocument9 pagesHirschprung DiseaseRajeev JhaNo ratings yet
- 9149StatlerMentalStatus PDFDocument5 pages9149StatlerMentalStatus PDFArumDesiPratiwiNo ratings yet
- Nursing Diagnoses Arranged by GordonDocument9 pagesNursing Diagnoses Arranged by GordonJoedeson Aroco BungubungNo ratings yet
- Ecology: of The Disease or Dynamic of Disease Transmission Chapter TwoDocument42 pagesEcology: of The Disease or Dynamic of Disease Transmission Chapter TwoCabdi WaliNo ratings yet
- Pathophysiology of Schizophrenia: February 2014Document24 pagesPathophysiology of Schizophrenia: February 2014Tuderici IoanaNo ratings yet
- Kr2med 2004engDocument49 pagesKr2med 2004engSuma LathaNo ratings yet
- Pathphys ModuleDocument102 pagesPathphys ModuleRodriguez Vivanco Kevin DanielNo ratings yet
- Colon Cancer Care Plan PDFDocument4 pagesColon Cancer Care Plan PDFTob JurNo ratings yet
- Ocd 1Document35 pagesOcd 1VARSHANo ratings yet
- Health AssessmentDocument18 pagesHealth AssessmentSavita Hanamsagar100% (1)
- Preoperative Preparation of The Surgical PatientDocument33 pagesPreoperative Preparation of The Surgical PatientPrincewill SeiyefaNo ratings yet
- mhGAP Humanitarian Intervention Guide (mhGAP-HIG) - English VersionDocument68 pagesmhGAP Humanitarian Intervention Guide (mhGAP-HIG) - English VersionПламен МинчевNo ratings yet
- NCM116 Module 3 Cerebrovascular Disease QuizDocument5 pagesNCM116 Module 3 Cerebrovascular Disease QuizIvan FernandezNo ratings yet
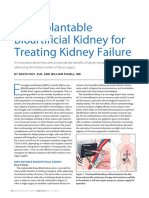
- An Implantable Bioartificial Kidney For Treating Kidney FailureDocument2 pagesAn Implantable Bioartificial Kidney For Treating Kidney FailureAnugrah Pangeran100% (1)
- TUBERCULOSIS (Lec Community Medicine)Document24 pagesTUBERCULOSIS (Lec Community Medicine)wanderer_1010No ratings yet
- Pa Tho Physiology of ParkinsonDocument2 pagesPa Tho Physiology of Parkinsoncuriosity_killsNo ratings yet
- 3 Schizophrenia AssessmentDocument36 pages3 Schizophrenia AssessmentArvindhanNo ratings yet
- A. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherDocument70 pagesA. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherMwansaay Twain HolyNo ratings yet
- Astigmatism: Nishita Afrin ICO B.OptomDocument41 pagesAstigmatism: Nishita Afrin ICO B.OptomClaudia SerbanNo ratings yet
- Case Presentation Second Year 2nd SemesterDocument36 pagesCase Presentation Second Year 2nd SemesterJohn Robert PescadorNo ratings yet
- G3 IAH and ACSDocument29 pagesG3 IAH and ACSRoshin Mae E. TejeroNo ratings yet
- Emergency Management of DKADocument12 pagesEmergency Management of DKAtinzioNo ratings yet
- Orchitis (Eng)Document15 pagesOrchitis (Eng)Ferzy Awwali FadhilaNo ratings yet
- Thrombolytics, Anticoags, Antiplatelets PDFDocument21 pagesThrombolytics, Anticoags, Antiplatelets PDFrachelkdoNo ratings yet
- Quiz 1Document3 pagesQuiz 1Wiljohn de la CruzNo ratings yet
- Heme Degradation & HyperbilirubinemiasDocument30 pagesHeme Degradation & HyperbilirubinemiasSubhi MishraNo ratings yet
- Cervical CA Case StudyDocument32 pagesCervical CA Case StudyCandy Mae Kabayao CuraNo ratings yet
- Patient ChartDocument2 pagesPatient ChartHydieNo ratings yet
- NCM116 Addison DiseaseDocument20 pagesNCM116 Addison DiseaseSofia MikaelaNo ratings yet
- AtaxiaDocument8 pagesAtaxiaDivya Gupta0% (1)
- Module 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - ClementeDocument27 pagesModule 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - Clementeelaine100% (1)
- Abdominal Thrust Maneuver - StatPearls - NCBI BookshelfDocument4 pagesAbdominal Thrust Maneuver - StatPearls - NCBI BookshelfberlianNo ratings yet
- Need Motivates The Behaviour of A Person.: Human Needs TheoryDocument8 pagesNeed Motivates The Behaviour of A Person.: Human Needs TheoryDan Ataniel EnsaladaNo ratings yet
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseasejustinahorroNo ratings yet
- "Monograph Eating Disorders": StudentDocument12 pages"Monograph Eating Disorders": StudentTeffy NeyraNo ratings yet
- (Osborn) Chapter 51: Learning Outcomes (Number and Title)Document16 pages(Osborn) Chapter 51: Learning Outcomes (Number and Title)KittiesNo ratings yet
- 1 Anaphylaxis Anaphylaxis Is A Life-Threatening TypeDocument9 pages1 Anaphylaxis Anaphylaxis Is A Life-Threatening TypeCraigNo ratings yet
- JurnalDocument11 pagesJurnaldewiulfaNo ratings yet
- Challenging Cell Phone Impact On Reproduction: A Review: Gonadal Physiology and DiseaseDocument5 pagesChallenging Cell Phone Impact On Reproduction: A Review: Gonadal Physiology and DiseasedewiulfaNo ratings yet
- SelectionDocument5 pagesSelectiondewiulfaNo ratings yet
- Jurnal 1Document12 pagesJurnal 1dewiulfaNo ratings yet
- Rini 2013 Against Infanticide J MeDocument8 pagesRini 2013 Against Infanticide J MedewiulfaNo ratings yet
- Regulus GreenDocument22 pagesRegulus GreenAnggiNo ratings yet
- Regulus GreenDocument22 pagesRegulus GreenAnggiNo ratings yet
- 09 (Optional) GLOMERULONEPHRITIS - DWI - FIN PDFDocument108 pages09 (Optional) GLOMERULONEPHRITIS - DWI - FIN PDFdewiulfaNo ratings yet
- Regulus GreenDocument22 pagesRegulus GreenAnggiNo ratings yet
- Regulus GreenDocument22 pagesRegulus GreenAnggiNo ratings yet
- RigelDocument52 pagesRigeldewiulfaNo ratings yet
- Sport Injury DR Endang AmbarwatiDocument44 pagesSport Injury DR Endang AmbarwatidewiulfaNo ratings yet
- RigelDocument52 pagesRigeldewiulfaNo ratings yet
- Musculoskeletal RehabilitationDocument25 pagesMusculoskeletal RehabilitationNadia Ayu TiarasariNo ratings yet
- Sport Injury DR Endang AmbarwatiDocument44 pagesSport Injury DR Endang AmbarwatidewiulfaNo ratings yet
- 2 Cells CommunicationDocument74 pages2 Cells CommunicationdewiulfaNo ratings yet
- DNA ReplicationDocument69 pagesDNA ReplicationdewiulfaNo ratings yet
- 3 Stem CellsDocument70 pages3 Stem CellsdewiulfaNo ratings yet
- Eukaryote Regulation of Gene ExpressionDocument35 pagesEukaryote Regulation of Gene ExpressiondewiulfaNo ratings yet
- 4 CELL INJURY - Nerosis Vs ApoptosisDocument64 pages4 CELL INJURY - Nerosis Vs ApoptosisdewiulfaNo ratings yet
- DNA Damage and RepairDocument47 pagesDNA Damage and RepairdewiulfaNo ratings yet
- 2 Cells CommunicationDocument74 pages2 Cells CommunicationdewiulfaNo ratings yet
- 1-2 PCR and Gel ElectrophoresisDocument22 pages1-2 PCR and Gel ElectrophoresisdewiulfaNo ratings yet
- 1-5 Genetic EngineeringDocument42 pages1-5 Genetic EngineeringdewiulfaNo ratings yet
- 1-4 DNA SequencingDocument90 pages1-4 DNA SequencingdewiulfaNo ratings yet
- English Grammar TensesDocument124 pagesEnglish Grammar TensesdewiulfaNo ratings yet
- DNA Extraction OverviewDocument14 pagesDNA Extraction OverviewNicholas SoNo ratings yet
- Examine Act 1 Scene 7Document6 pagesExamine Act 1 Scene 7callummeliaNo ratings yet
- Slang WordsDocument32 pagesSlang WordsJuanjo HornoNo ratings yet
- Get A Knife Get A Dog, But Get Rid of Gun'sDocument2 pagesGet A Knife Get A Dog, But Get Rid of Gun'sACADEMICVENUE100% (1)
- Crimlaw CasesDocument7 pagesCrimlaw Casesxerah0808No ratings yet
- Crime Scene PhotoDocument4 pagesCrime Scene PhotoLhine KiwalanNo ratings yet
- Complete Criminal Law Bennett For MyersDocument15 pagesComplete Criminal Law Bennett For MyersDewey Bennett100% (2)
- Macbeth - Entire PlayDocument86 pagesMacbeth - Entire PlayShaimaa SuleimanNo ratings yet
- Martin Bidney EpiphanologyDocument26 pagesMartin Bidney EpiphanologyDana KiosaNo ratings yet
- Revised Ortega Lecture Notes IIDocument191 pagesRevised Ortega Lecture Notes IIPanzer OverlordNo ratings yet
- New Ob W Crimes TestDocument9 pagesNew Ob W Crimes TestIsabella Martinetti Khamg0% (1)
- AbcdDocument5 pagesAbcdaustinederick606100% (1)
- Macbeth .Critica, Genero y Tragedia Del Ser Humano, 2007 PDFDocument18 pagesMacbeth .Critica, Genero y Tragedia Del Ser Humano, 2007 PDFpapelerito100% (1)
- Ponce Wanted Poster EnglishDocument1 pagePonce Wanted Poster EnglishAnonymous hTA0wKPm7No ratings yet
- The Unlucky Theatre 2014-1Document3 pagesThe Unlucky Theatre 2014-1OctavioMonCa100% (1)
- They Must Be Alleged. Otherwise, They Will Not Be CredibleDocument8 pagesThey Must Be Alleged. Otherwise, They Will Not Be CrediblemmaNo ratings yet
- OIS BowmanDocument29 pagesOIS BowmanReno Gazette JournalNo ratings yet
- Legal Writing: de Jesus, Tracy Ann de Torres, RechelDocument17 pagesLegal Writing: de Jesus, Tracy Ann de Torres, RechelRechel De TorresNo ratings yet
- Murder Robbery Homicide Case Police BlotterDocument11 pagesMurder Robbery Homicide Case Police BlotterBilly Elago Maghirang100% (1)
- Ethical Dilemmas CasesDocument10 pagesEthical Dilemmas CasesAreiyneYhêlleBaculioHamacNo ratings yet
- The FalconerDocument58 pagesThe FalconerChronicleBooks100% (1)
- Case CrimDocument3 pagesCase CrimRochelle Ann ReyesNo ratings yet
- OJ Simpson PDFDocument36 pagesOJ Simpson PDFcatNo ratings yet
- People Vs TeehankeeDocument3 pagesPeople Vs TeehankeekhailcalebNo ratings yet
- Ogden 2006Document16 pagesOgden 2006A.VictorNo ratings yet
- Juan Fernando HermosaDocument2 pagesJuan Fernando HermosaMegan Lucy HarrisonNo ratings yet
- Police Affidavit For The Arrest of Chandler Ari DunmeyerDocument1 pagePolice Affidavit For The Arrest of Chandler Ari DunmeyerABC15 NewsNo ratings yet
- Story of The Lady BluebeardDocument7 pagesStory of The Lady BluebeardKriti SethiNo ratings yet
- Rowland v. StateDocument2 pagesRowland v. Statecrlstinaaa50% (2)
- Criminal LawDocument313 pagesCriminal LawAbhimanyu Singh100% (1)
- Gun Violence: Lesson Plan: TopicDocument4 pagesGun Violence: Lesson Plan: TopicWilliam WrightNo ratings yet