You might also like
- Lampiran E8 MATRIKS SIKA, TANGGUNG JAWAB INSIDEN DAN DAMPAK PEKERJAAN NON PEMBORANDocument5 pagesLampiran E8 MATRIKS SIKA, TANGGUNG JAWAB INSIDEN DAN DAMPAK PEKERJAAN NON PEMBORANsamsul zamaniNo ratings yet
- FORM HSE MATRIX TRAINING (Contoh)Document1 pageFORM HSE MATRIX TRAINING (Contoh)Hifni GhazaliNo ratings yet
- Cobain PpliDocument15 pagesCobain Pplipras husein29No ratings yet
- IDENTIFIKASI SUMBER BAHAYA DI TEMPAT KERJA PT INDO VENEER UTAMADocument19 pagesIDENTIFIKASI SUMBER BAHAYA DI TEMPAT KERJA PT INDO VENEER UTAMAAjiWidyartaNo ratings yet
- Pekerjaan Pembangunan Terminal LPG Refrigerated Jawa Timur (Lingkup Pekerjaan Site Development, Pagar Dan LPG Storage Tank)Document1 pagePekerjaan Pembangunan Terminal LPG Refrigerated Jawa Timur (Lingkup Pekerjaan Site Development, Pagar Dan LPG Storage Tank)Ajie Dwi YuniarsoNo ratings yet
- HR VISION AND MISSION STATEMENTSDocument18 pagesHR VISION AND MISSION STATEMENTSahashujanNo ratings yet
- Matriks Training LK3Document6 pagesMatriks Training LK3Ahmad Iqbal LazuardiNo ratings yet
- Example Risk Assessment For Outdoor EventsDocument6 pagesExample Risk Assessment For Outdoor EventsAnonymous 5YMOxVQNo ratings yet
- HSE Officer Job at Grand IndonesiaDocument2 pagesHSE Officer Job at Grand IndonesiaKontan Nauval AlifianNo ratings yet
- KPI TAM BP Surabaya Kenjeran 12desemberDocument15 pagesKPI TAM BP Surabaya Kenjeran 12desemberBP SuroboyoNo ratings yet
- Subcontractor Production Report: Job SafetyDocument2 pagesSubcontractor Production Report: Job Safetyzubair nawazNo ratings yet
- Appraisal EmployeeDocument4 pagesAppraisal EmployeeAdi Sutrisno100% (1)
- Intent: - : Safety Shoe PolicyDocument2 pagesIntent: - : Safety Shoe Policyvenkat100% (1)
- Employee Skill MatrixDocument2 pagesEmployee Skill MatrixBUdiNo ratings yet
- STR GL Hal Hse SQ 501Document12 pagesSTR GL Hal Hse SQ 501jose gregorio mata cabezaNo ratings yet
- HSE Training Superintendent RoleDocument3 pagesHSE Training Superintendent RoleTLK ChannelNo ratings yet
- KTC Monthly Meeting Status UpdateDocument3 pagesKTC Monthly Meeting Status UpdateAzhar ArisNo ratings yet
- HSE Safety AuditsDocument3 pagesHSE Safety Auditsvlad100% (1)
- ASAB PHASE II (STAGE 2) FIELD DEVELOPMENT PROJECT HSE TRAININGDocument1 pageASAB PHASE II (STAGE 2) FIELD DEVELOPMENT PROJECT HSE TRAININGmoonlidht edithNo ratings yet
- MatrixDocument1 pageMatrixRengga PramadyaksaNo ratings yet
- Standard Operating Procedure Ref 162Document3 pagesStandard Operating Procedure Ref 162RilySabanaNo ratings yet
- Supervisors Safety Accountability ProgramDocument2 pagesSupervisors Safety Accountability ProgramcumminkNo ratings yet
- Competency Matrix For Technical StaffDocument1 pageCompetency Matrix For Technical StaffPasinduAlwisNo ratings yet
- Driving On SiteDocument15 pagesDriving On SitejhoniNo ratings yet
- 3 - OM & Other Functional Areas PDFDocument6 pages3 - OM & Other Functional Areas PDFSnehil KrNo ratings yet
- Driver Safety MEDocument7 pagesDriver Safety MEyahiyaNo ratings yet
- EMS training matrixDocument1 pageEMS training matrixhelgatheresaNo ratings yet
- KPIs For Finance & Accounting ManagerDocument5 pagesKPIs For Finance & Accounting Managervmglenn.ivcNo ratings yet
- Departmetit: Malrtehance Cost t5% Expenditurc BudsetDocument1 pageDepartmetit: Malrtehance Cost t5% Expenditurc Budsetrobby damanikNo ratings yet
- Staff Performance ReviewDocument3 pagesStaff Performance Reviewhima kiran kondapavuluriNo ratings yet
- Training Effectiveness Evaluation: Trainee's Evaluation (To Be Conducted Right After The Training)Document25 pagesTraining Effectiveness Evaluation: Trainee's Evaluation (To Be Conducted Right After The Training)shirwen ClamNo ratings yet
- HRM-04-0025 New Employee OrientationDocument3 pagesHRM-04-0025 New Employee Orientationandruta1978No ratings yet
- STUDENT GUIDE FOR COMPUTER SYSTEMS SERVICING NC IIDocument11 pagesSTUDENT GUIDE FOR COMPUTER SYSTEMS SERVICING NC IIAireen Letana SiagaNo ratings yet
- JSA-Substructure Concrete WorksDocument5 pagesJSA-Substructure Concrete WorksUMUTNo ratings yet
- Drawing Grating 25mmDocument1 pageDrawing Grating 25mmEko Wahyu QrakerNo ratings yet
- Excavation Permit FormDocument2 pagesExcavation Permit FormKarim KachourNo ratings yet
- Pdfslide - Us Jsa For Using Jack HammerDocument3 pagesPdfslide - Us Jsa For Using Jack HammerWidya BungaNo ratings yet
- HR Business Partner Job DescriptionDocument2 pagesHR Business Partner Job DescriptionPahala Simanjuntak100% (1)
- Occupational Health, Safety &: Issue Date: June 2013Document34 pagesOccupational Health, Safety &: Issue Date: June 2013Orchie DavidNo ratings yet
- Safety Goals & Objectives PT Indofood CBP Sukses Makmur TBK Cabang Semarang Tahun 2016Document7 pagesSafety Goals & Objectives PT Indofood CBP Sukses Makmur TBK Cabang Semarang Tahun 2016Emirza Nur WicaksonoNo ratings yet
- Confined Space Log SheetDocument1 pageConfined Space Log SheetRenatoNo ratings yet
- Form Report Safety CampaignDocument1 pageForm Report Safety CampaignErlan Gus HermawanNo ratings yet
- LOTO ChecklistDocument3 pagesLOTO ChecklistPutri UnaNo ratings yet
- Balance Score Card-NeedDocument36 pagesBalance Score Card-NeedParamjit Sharma100% (13)
- Matrix TrainingDocument5 pagesMatrix TrainingRengga PramadyaksaNo ratings yet
- Standarisasi Matrix Training Karyawan Pt. XXXXXXXXX: NO Materi/ItemDocument1 pageStandarisasi Matrix Training Karyawan Pt. XXXXXXXXX: NO Materi/Itemakbars.thasimaNo ratings yet
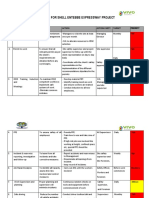
- Hsse Plan For Shell Entebbe Expressway Project: No Description Objective Action Action Party Target PriorityDocument5 pagesHsse Plan For Shell Entebbe Expressway Project: No Description Objective Action Action Party Target PriorityDENISNo ratings yet
- New Action Plan HK 2020Document1 pageNew Action Plan HK 2020Ruli Untaryo100% (1)
- Hse Training Plan Template ExcelDocument2 pagesHse Training Plan Template ExcelNasri matar0% (1)
- KYT and HHTDocument2 pagesKYT and HHTGURMUKH SINGHNo ratings yet
- B. Training MatrixDocument5 pagesB. Training MatrixwidiNo ratings yet
- Human Resource (HR) Policies and ProceduresDocument4 pagesHuman Resource (HR) Policies and ProceduresDanish NawazNo ratings yet
- 06-June Monthly QHSE PerformanceDocument11 pages06-June Monthly QHSE Performancemknkjbk kkjkNo ratings yet
- 360 Degree Performance Appraisal FormDocument6 pages360 Degree Performance Appraisal FormPhillip Miler100% (1)
- Employee Safety Training Matrix Template ExcelDocument79 pagesEmployee Safety Training Matrix Template ExcelRandy PedrozaNo ratings yet
- Contoh Tools Struktur Skala UpahDocument47 pagesContoh Tools Struktur Skala UpahNovanNo ratings yet
- 1 23 Forklift SafetyDocument4 pages1 23 Forklift SafetykhurramNo ratings yet
- Stop Work Report for Safety InterventionsDocument1 pageStop Work Report for Safety InterventionsRetselisitsoeNo ratings yet
- Announcement: Philippine Drug Enforcement AgencyDocument1 pageAnnouncement: Philippine Drug Enforcement AgencyErwin CalderonNo ratings yet
- HSE Training Plan - 2023Document1 pageHSE Training Plan - 2023adeeb zahidNo ratings yet
- Rash YuandriDocument1 pageRash YuandriadecNo ratings yet
- First Aid at Work PDFDocument1 pageFirst Aid at Work PDFadecNo ratings yet
- Captain America Papercraft Toy Paper CraftDocument1 pageCaptain America Papercraft Toy Paper CraftadecNo ratings yet
- First Aid at Work PDFDocument1 pageFirst Aid at Work PDFadecNo ratings yet
- First Aid Training Jakarta GuideDocument1 pageFirst Aid Training Jakarta GuideadecNo ratings yet
- Haz Id Poster1Document1 pageHaz Id Poster1AmeenudeenNo ratings yet
- Form Safety SignDocument1 pageForm Safety SignadecNo ratings yet
- Form Sign FormatDocument1 pageForm Sign FormatadecNo ratings yet
- Form Safety SignDocument1 pageForm Safety SignadecNo ratings yet
- What To Do in Medical Emergency Situation: © Chevron 2007Document7 pagesWhat To Do in Medical Emergency Situation: © Chevron 2007adecNo ratings yet
- First Aid at Work PDFDocument1 pageFirst Aid at Work PDFadecNo ratings yet
- Internal Production Use. If You Comply With The Rest of These License TermsDocument4 pagesInternal Production Use. If You Comply With The Rest of These License TermsadecNo ratings yet
- Internal Production Use. If You Comply With The Rest of These License TermsDocument4 pagesInternal Production Use. If You Comply With The Rest of These License TermsadecNo ratings yet
- Internal Production Use. If You Comply With The Rest of These License TermsDocument4 pagesInternal Production Use. If You Comply With The Rest of These License TermsadecNo ratings yet
- Internal Production Use. If You Comply With The Rest of These License TermsDocument4 pagesInternal Production Use. If You Comply With The Rest of These License TermsadecNo ratings yet
- Internal Production Use. If You Comply With The Rest of These License TermsDocument4 pagesInternal Production Use. If You Comply With The Rest of These License TermsadecNo ratings yet
- Kerry Washington. Family Secret.Document3 pagesKerry Washington. Family Secret.yulya.shevchenko110No ratings yet
- Marriage and Later PartDocument25 pagesMarriage and Later PartDeepak PoudelNo ratings yet
- Progress Test 04Document6 pagesProgress Test 04Lemmy the GamerNo ratings yet
- DRRM Plan2020 2021Document5 pagesDRRM Plan2020 2021SheChanNo ratings yet
- My Good Habits - Welcome Booklet 2 - 1Document17 pagesMy Good Habits - Welcome Booklet 2 - 1lisa_ernsbergerNo ratings yet
- Research Paper 4Document26 pagesResearch Paper 4Amit RajputNo ratings yet
- Csa Fodrea 2014 - 2015 Student Handbook FinalDocument37 pagesCsa Fodrea 2014 - 2015 Student Handbook Finalapi-260407035No ratings yet
- MHFL Functional FoodsDocument24 pagesMHFL Functional FoodsZekel HealthcareNo ratings yet
- Working Heights Fall Arrest Systems PDFDocument4 pagesWorking Heights Fall Arrest Systems PDFPraful E. PawarNo ratings yet
- Senior Counsel or Associate General Counsel or Assistant GeneralDocument3 pagesSenior Counsel or Associate General Counsel or Assistant Generalapi-76922317No ratings yet
- ASHRAE Std 62.1 Ventilation StandardDocument38 pagesASHRAE Std 62.1 Ventilation Standardcoolth2No ratings yet
- P3DOC001346 - ISSUE - G MSDS HAFEX EnglishDocument10 pagesP3DOC001346 - ISSUE - G MSDS HAFEX EnglishOperations AdminNo ratings yet
- Surgical Instruments and Drains PDFDocument117 pagesSurgical Instruments and Drains PDFNariska CooperNo ratings yet
- Lateral SMASectomy FaceliftDocument8 pagesLateral SMASectomy FaceliftLê Minh KhôiNo ratings yet
- UWI-Mona 2021-2022 Graduate Fee Schedule (July 2021)Document15 pagesUWI-Mona 2021-2022 Graduate Fee Schedule (July 2021)Akinlabi HendricksNo ratings yet
- Sulphonamides: A Pharmaceutical ReviewDocument3 pagesSulphonamides: A Pharmaceutical ReviewinventionjournalsNo ratings yet
- The Effectiveness of Community-Based Rehabilitation Programs For Person Who Use Drugs (PWUD) : Perspectives of Rehabilitation Care Workers in IloiloDocument27 pagesThe Effectiveness of Community-Based Rehabilitation Programs For Person Who Use Drugs (PWUD) : Perspectives of Rehabilitation Care Workers in IloiloErikah Eirah BeloriaNo ratings yet
- Staples Worklife Magazine - Winter 2019Document68 pagesStaples Worklife Magazine - Winter 2019Anonymous fq268KsS100% (1)
- Metaphor and MedicineDocument9 pagesMetaphor and MedicineCrystal DuarteNo ratings yet
- The Regent's Park - Risk AssessmentDocument3 pagesThe Regent's Park - Risk AssessmentEiman'E'RostamiNo ratings yet
- F&F LetterDocument3 pagesF&F LetterJaskeerat Singh50% (2)
- Stok Benang Kamar OperasiDocument5 pagesStok Benang Kamar OperasirendyNo ratings yet
- Which Is More Effective in Treating Chronic Stable Angina, Trimetazidine or Diltiazem?Document5 pagesWhich Is More Effective in Treating Chronic Stable Angina, Trimetazidine or Diltiazem?Lemuel Glenn BautistaNo ratings yet
- HAV IgG/IgM Test InstructionsDocument2 pagesHAV IgG/IgM Test InstructionsRuben DuranNo ratings yet
- IPAMS Healthcare and Medical Services Evaluation FormDocument2 pagesIPAMS Healthcare and Medical Services Evaluation FormManases VelasquezNo ratings yet
- TOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaDocument24 pagesTOFPA: A Surgical Approach To Tetralogy of Fallot With Pulmonary AtresiaRedmond P. Burke MD100% (1)
- Complications of Caesarean Section: ReviewDocument8 pagesComplications of Caesarean Section: ReviewDesi Purnamasari YanwarNo ratings yet
- AFP Hemoptysis - 2022Document9 pagesAFP Hemoptysis - 2022Joshua DiaoNo ratings yet
- Agile Project Management: Course 4. Agile Leadership Principles and Practices Module 3 of 4Document32 pagesAgile Project Management: Course 4. Agile Leadership Principles and Practices Module 3 of 4John BenderNo ratings yet
- MSDS Material Safety Data Sheet Decon 90 CleanerDocument4 pagesMSDS Material Safety Data Sheet Decon 90 CleanerNorman LeungNo ratings yet