You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Rhesus (RH) Blood Group SystemDocument44 pagesThe Rhesus (RH) Blood Group SystemMarl EstradaNo ratings yet
- After Effects of COVID 19 and Repair of LungsDocument13 pagesAfter Effects of COVID 19 and Repair of LungsAthenaeum Scientific PublishersNo ratings yet
- S8 - End-of-Unit 1 TestDocument2 pagesS8 - End-of-Unit 1 TestWilliam Anthony56% (9)
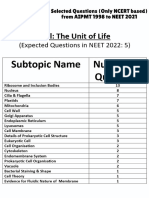
- Cell - The Unit of Life - NCERT Based PYQsDocument9 pagesCell - The Unit of Life - NCERT Based PYQsAkhil singhNo ratings yet
- ) Science (Department: Grade (10) Final Revision Worksheet (Biology)Document13 pages) Science (Department: Grade (10) Final Revision Worksheet (Biology)Toto BjNo ratings yet
- Human Body WorksheetsDocument20 pagesHuman Body Worksheetsnona wayne dela peñaNo ratings yet
- Sensory and Motor Nerve EndingsDocument42 pagesSensory and Motor Nerve EndingsMark GanirNo ratings yet
- Cytoskeleton and The ComponentsDocument1 pageCytoskeleton and The ComponentsTisha TabhitaNo ratings yet
- Association Between Battledore Placenta and Perinatal ComplicationDocument3 pagesAssociation Between Battledore Placenta and Perinatal Complicationtipu42No ratings yet
- The Morphology of The Post-Gastric Alimentary CanalDocument18 pagesThe Morphology of The Post-Gastric Alimentary CanalAnca MihalcescuNo ratings yet
- Multiple Myeloma: NCCN Guidelines For PatientsDocument78 pagesMultiple Myeloma: NCCN Guidelines For PatientsAchmad Farodisi AfnaniNo ratings yet
- Veterinary DermatologyDocument1 pageVeterinary DermatologyCiolacu Victor AdrianNo ratings yet
- Pengaruh Pemberian Terapi Latihan Metode SchrothDocument7 pagesPengaruh Pemberian Terapi Latihan Metode SchrothsulaimanNo ratings yet
- Anatomy and Physiology of The AirwayDocument42 pagesAnatomy and Physiology of The Airwayiaa100% (1)
- Chronic Expanding Hematoma Following AbdominoplastyDocument4 pagesChronic Expanding Hematoma Following AbdominoplastyGabriela Serra del CarpioNo ratings yet
- Part of BodyDocument4 pagesPart of Bodyanon_535068952No ratings yet
- Latin For AnatomyDocument4 pagesLatin For AnatomyAchraf RabadiNo ratings yet
- Final Exam Review SheetDocument2 pagesFinal Exam Review Sheetapi-264668182No ratings yet
- Ceva NecropsyDocument18 pagesCeva NecropsyNanda Ayu Cindy KashiwabaraNo ratings yet
- The - Skeletal - System Lab ActDocument13 pagesThe - Skeletal - System Lab Actwelfred indinoNo ratings yet
- CH 14 Brain & Cranial NervesDocument37 pagesCH 14 Brain & Cranial NervesHeather LaurenNo ratings yet
- Anatomy and Physiology of The Respiratory SystemDocument5 pagesAnatomy and Physiology of The Respiratory SystemxoxosvwNo ratings yet
- Collection, Preservation and Submission of Sample To The Microbiology LaboratoryDocument26 pagesCollection, Preservation and Submission of Sample To The Microbiology LaboratoryDrRajkumar PatelNo ratings yet
- Pathologic Basis of Veterinary Disease 7Th Edition James F Zachary Full Chapter PDF ScribdDocument67 pagesPathologic Basis of Veterinary Disease 7Th Edition James F Zachary Full Chapter PDF Scribdtodd.feuer645100% (6)
- Organoids On CHipDocument7 pagesOrganoids On CHipAvtar JephNo ratings yet
- 1.4 Selecton of Blood BagDocument3 pages1.4 Selecton of Blood BagBALAJINo ratings yet
- Campbells Operative Orthopaedics 4 Volume Set Elsevier 2020 Frederick M Azar Full ChapterDocument67 pagesCampbells Operative Orthopaedics 4 Volume Set Elsevier 2020 Frederick M Azar Full Chapteredith.beltran702100% (5)
- Frog Dissection (Remote)Document21 pagesFrog Dissection (Remote)Mohammad NiyaifarNo ratings yet
- Therapeutic Apheresis Operator Competency Aug06Document43 pagesTherapeutic Apheresis Operator Competency Aug06Jose Gregorio Riobueno BolivarNo ratings yet
- Call of Cthulhu - 1990 - Delta Green - Handout - Deep One AutopsyDocument2 pagesCall of Cthulhu - 1990 - Delta Green - Handout - Deep One AutopsyFeartherNo ratings yet