You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Abstract DwicitDocument1 pageAbstract DwicitJihan Anandya Alyka FitriNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Abstract DwicitDocument1 pageAbstract DwicitJihan Anandya Alyka FitriNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Abstract DwicitDocument1 pageAbstract DwicitJihan Anandya Alyka FitriNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Gastroenterology Research and PracticeDocument19 pagesGastroenterology Research and PracticeJihan Anandya Alyka FitriNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- JRDocument16 pagesJRJihan Anandya Alyka FitriNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Undangan Festival Serakal BarzanjiDocument4 pagesUndangan Festival Serakal BarzanjiJihan Anandya Alyka FitriNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Undangan Festival Serakal BarzanjiDocument4 pagesUndangan Festival Serakal BarzanjiJihan Anandya Alyka FitriNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Undangan Festival Serakal BarzanjiDocument4 pagesUndangan Festival Serakal BarzanjiJihan Anandya Alyka FitriNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Therapeutics Handbook 2014 - 140804Document384 pagesTherapeutics Handbook 2014 - 140804Eriet HidayatNo ratings yet
- AAPCDocument10 pagesAAPCprincyphilip67% (3)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Medical Device Reports Medical Device Vigilance SystemsDocument15 pagesMedical Device Reports Medical Device Vigilance Systemshitham shehataNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Venosmil Technical NformationDocument6 pagesVenosmil Technical NformationTheo HemagiriNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Nursing Diagnosis: Acute Pain: NANDA Definition: Pain Is Whatever The ExperiencingDocument13 pagesNursing Diagnosis: Acute Pain: NANDA Definition: Pain Is Whatever The Experiencingasmika danaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- SAS Proc Report at WorkDocument43 pagesSAS Proc Report at WorkNimit Mohan NarsipurNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Causality AssessmentDocument2 pagesCausality AssessmentromeoqfacebookNo ratings yet
- Nurse's Role and Responsibilities in Administration of MedicationDocument88 pagesNurse's Role and Responsibilities in Administration of MedicationSonia Singh88% (33)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Clozapine Initiation and MaintenanceDocument15 pagesClozapine Initiation and MaintenanceDiana LasluizaNo ratings yet
- Medication Competency Assessment MC002Document48 pagesMedication Competency Assessment MC002Ameng GosimNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Statins and Succinylcholine InteractionDocument5 pagesStatins and Succinylcholine InteractionaksinuNo ratings yet
- Pharmacology Reasons and Effect On SocietyDocument7 pagesPharmacology Reasons and Effect On SocietyAlejandro Arévalo RamosNo ratings yet
- PharmacotherapyDocument15 pagesPharmacotherapyPrincess RonsableNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
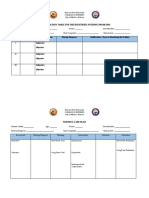
- Prioritization Table For The Identified Nursing ProblemsDocument3 pagesPrioritization Table For The Identified Nursing ProblemsMia PascualNo ratings yet
- 1a EVOLVE-CARE PLAN CONSTRUCTOR TUTORIALDocument4 pages1a EVOLVE-CARE PLAN CONSTRUCTOR TUTORIALdavidvpnNo ratings yet
- NeostigmineDocument4 pagesNeostigmineDonna Lyn B. DizonNo ratings yet
- I. Pharmacist's Workup of Drug Therapy For Bronchial AsthmaDocument7 pagesI. Pharmacist's Workup of Drug Therapy For Bronchial AsthmaDave Cabuyadao0% (1)
- First Aid For Drug OverdoseDocument6 pagesFirst Aid For Drug OverdoseJason ArellanoNo ratings yet
- CefuroximeDocument14 pagesCefuroximeBentoys StreetNo ratings yet
- Egyptian Guideline On ADR Reporting For Healthcare Professionals 15-12-2011 Version 01Document29 pagesEgyptian Guideline On ADR Reporting For Healthcare Professionals 15-12-2011 Version 01Hanan AhmedNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- 08 31 16 Drug Information ResourcesDocument73 pages08 31 16 Drug Information ResourcesSandra BaiNo ratings yet
- Hypodermoclysis: A Literature Review To Assist in Clinical PracticeDocument7 pagesHypodermoclysis: A Literature Review To Assist in Clinical PracticeRaabe AndradeNo ratings yet
- Famotidine (Pepcid)Document1 pageFamotidine (Pepcid)Cassie100% (1)
- FluidooperationDocument35 pagesFluidooperationmohammad khlaifatNo ratings yet
- Luspatercept FDA Approval Press Release - FINALDocument6 pagesLuspatercept FDA Approval Press Release - FINALBazz UkkyNo ratings yet
- Herbal Beverage PDFDocument12 pagesHerbal Beverage PDFchen mee LimNo ratings yet
- Early Mobility and Walking For Patients With Femoral Arterial Catheters in Intensive Care Unit: A Case SeriesDocument5 pagesEarly Mobility and Walking For Patients With Femoral Arterial Catheters in Intensive Care Unit: A Case Seriesapi-240991897No ratings yet
- Adr Form 10Document3 pagesAdr Form 10doctor uroosaNo ratings yet
- Exploring The Combination and Modular Characteristics of Herbs For Alopecia Treatment in Traditional Chinese Medicine: An Association Rule Mining and Network Analysis StudyDocument13 pagesExploring The Combination and Modular Characteristics of Herbs For Alopecia Treatment in Traditional Chinese Medicine: An Association Rule Mining and Network Analysis StudyRenata AlbuquerqueNo ratings yet
- Drug Exception Application 04-14 EDocument3 pagesDrug Exception Application 04-14 Econtext-tines-0eNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)