You might also like
- Employee Confidentiality and Non-Disclosure AgreementDocument5 pagesEmployee Confidentiality and Non-Disclosure AgreementshamoojeeNo ratings yet
- How To Text A Girl - A Girls Chase Guide (Girls Chase Guides) (PDFDrive) - 31-61Document31 pagesHow To Text A Girl - A Girls Chase Guide (Girls Chase Guides) (PDFDrive) - 31-61Myster HighNo ratings yet
- THE DOSE, Issue 1 (Tokyo)Document142 pagesTHE DOSE, Issue 1 (Tokyo)Damage85% (20)
- Airpax Series 5024 Temperature SensorsDocument2 pagesAirpax Series 5024 Temperature SensorsakaNo ratings yet
- Oxgen Sensor Cat WEBDocument184 pagesOxgen Sensor Cat WEBBuddy Davis100% (2)
- Gencomm 16 07 2020Document276 pagesGencomm 16 07 2020operaciones1 sesaNo ratings yet
- Resume - Yogesh Kumar - BSS Lead - Project LeadDocument5 pagesResume - Yogesh Kumar - BSS Lead - Project LeadharyantojogjaboyNo ratings yet
- EM 6400 DigitAN Register MapDocument10 pagesEM 6400 DigitAN Register MapAnoop Kumar PandayNo ratings yet
- GE Multilin MM300 Instruction ManualDocument195 pagesGE Multilin MM300 Instruction ManualDiego CastañedaNo ratings yet
- 3BSE020923R4101 A en S800 I O - General Information and Installation - User S GuideDocument256 pages3BSE020923R4101 A en S800 I O - General Information and Installation - User S GuideRavenShieldXNo ratings yet
- Business Case PresentationDocument27 pagesBusiness Case Presentationapi-253435256No ratings yet
- Marshall Stability Test AnalysisDocument5 pagesMarshall Stability Test AnalysisZick Zickry50% (2)
- GFK1533-VersaMax DeviceNet Communication ModulesDocument54 pagesGFK1533-VersaMax DeviceNet Communication ModulesSantosh GopalNo ratings yet
- CDVR 6Document4 pagesCDVR 6wagner_guimarães_1100% (1)
- Mrs. Universe PH - Empowering Women, Inspiring ChildrenDocument2 pagesMrs. Universe PH - Empowering Women, Inspiring ChildrenKate PestanasNo ratings yet
- Surgearresters Monitoring Eng Final PDFDocument12 pagesSurgearresters Monitoring Eng Final PDFCao Thanh TuanNo ratings yet
- C SoftwareDocument62 pagesC SoftwareJimmy ContarinoNo ratings yet
- CitectSCADA - Quick Start Tutorial - Part 1Document89 pagesCitectSCADA - Quick Start Tutorial - Part 1Adit GilaNo ratings yet
- A8000 To SCC 104 ConfigurationDocument6 pagesA8000 To SCC 104 ConfigurationAjith MerinNo ratings yet
- UnidriveDocument102 pagesUnidriveJuan Martín Luna MártirNo ratings yet
- SDG Implementers GuideDocument260 pagesSDG Implementers GuideJeevanandhamNo ratings yet
- ASE2000 Version 2 DNP3 Certification ProceduresDocument17 pagesASE2000 Version 2 DNP3 Certification ProceduresglizzanoNo ratings yet
- User Manual: ETP48200-C5B4 and ETP48200-C5B5 Embedded PowerDocument93 pagesUser Manual: ETP48200-C5B4 and ETP48200-C5B5 Embedded PowerDmitry059No ratings yet
- Installation Instructions For The FT-10 Network Genset LonWorks Card With PCC3200Document7 pagesInstallation Instructions For The FT-10 Network Genset LonWorks Card With PCC3200Nguyen SonNo ratings yet
- Dief - AGC 222 - Details of The Synch and Protection RelayDocument29 pagesDief - AGC 222 - Details of The Synch and Protection RelayT.S. AnklesariaNo ratings yet
- InteliMains 210 BTB 2 0 0 Global GuideDocument576 pagesInteliMains 210 BTB 2 0 0 Global GuideNatan Genao HdezNo ratings yet
- XCell Equipment User Guide 2.01Document49 pagesXCell Equipment User Guide 2.01Aline Camurate BarbosaNo ratings yet
- Option N Modbus TCP IPDocument32 pagesOption N Modbus TCP IPJosé Miguel Echeverria HerediaNo ratings yet
- Gencomm Alarms: Dsegencomm ProtocolDocument12 pagesGencomm Alarms: Dsegencomm ProtocolFariz Nur100% (1)
- Manual ProtoCessorDocument33 pagesManual ProtoCessorjohaquin loveNo ratings yet
- Ref 542 Plus Installation CommissioningDocument80 pagesRef 542 Plus Installation CommissioningMasrurul Azni Abdul AzizNo ratings yet
- Continuum+Security+Family Andover ControlsDocument20 pagesContinuum+Security+Family Andover ControlspujFierrosNo ratings yet
- FX0 30MRDocument69 pagesFX0 30MRkhangbao07No ratings yet
- 3BDD012903-600 A en AC 800M 6.0 FOUNDATION Fieldbus HSE PDFDocument152 pages3BDD012903-600 A en AC 800M 6.0 FOUNDATION Fieldbus HSE PDFtimsar1357No ratings yet
- SICAM A8000 - HMI - ProfileDocument2 pagesSICAM A8000 - HMI - ProfileChristian Vasquez MedranoNo ratings yet
- 57-606.9 Eclipse Model 706 Hart Io 1 PDFDocument108 pages57-606.9 Eclipse Model 706 Hart Io 1 PDFAbdul Shaharlal ENo ratings yet
- YK PSW3kVA 2U Rack Mount Inverter 3kVA Datasheet v1.6Document2 pagesYK PSW3kVA 2U Rack Mount Inverter 3kVA Datasheet v1.6Dr.Ahmed GhareebNo ratings yet
- Antidote IEEE 11073-20601 Library Developers GuideDocument23 pagesAntidote IEEE 11073-20601 Library Developers Guidekeyz182No ratings yet
- Easergy Builder en Rev1.3 104Document114 pagesEasergy Builder en Rev1.3 104alex pardoNo ratings yet
- GE Fanuc Automation: Cimplicity Hmi Important Product InformationDocument40 pagesGE Fanuc Automation: Cimplicity Hmi Important Product InformationSanjeev NairNo ratings yet
- Sicam PDocument16 pagesSicam PFlo Mirca100% (1)
- Introduction To T&T ElevatorsDocument48 pagesIntroduction To T&T ElevatorsEldho unni vargheseNo ratings yet
- Application Reverse Osmosis DOC en PDFDocument93 pagesApplication Reverse Osmosis DOC en PDFfernandoNo ratings yet
- TDS-100M ManualDocument24 pagesTDS-100M ManualjjrondonrNo ratings yet
- Parking Cooler System Nitecool Tcc-100: Installation and Service InstructionsDocument12 pagesParking Cooler System Nitecool Tcc-100: Installation and Service Instructionsebuk123No ratings yet
- Pacsystems Rx3I & Rsti-Ep Profinet Io-Controller User ManualDocument169 pagesPacsystems Rx3I & Rsti-Ep Profinet Io-Controller User ManualJulio Cesar Perez NavarroNo ratings yet
- Telecom Energy Brochure - 3T190225-V1 (电子档)Document14 pagesTelecom Energy Brochure - 3T190225-V1 (电子档)Franklin Fernandez100% (1)
- CEMPLE Users Guide, TriStation v3.0 PDFDocument100 pagesCEMPLE Users Guide, TriStation v3.0 PDFMohamed AmineNo ratings yet
- Be142 Genset Controller ManualDocument28 pagesBe142 Genset Controller ManualSousaFVNo ratings yet
- G120 - Parameter List PDFDocument416 pagesG120 - Parameter List PDFNikhil TripathiNo ratings yet
- M-Cubed Installation Procedure R1.8Document17 pagesM-Cubed Installation Procedure R1.8Srinath Gopala KrishnaNo ratings yet
- Datasheet SYNC 2000Document2 pagesDatasheet SYNC 2000Sharp Ta NoeNo ratings yet
- Csyc12mkf Service ManualDocument71 pagesCsyc12mkf Service ManualcoronaqcNo ratings yet
- EST3 Installation and Service ManualDocument386 pagesEST3 Installation and Service ManualБахтияр ЮмачиковNo ratings yet
- Custom Modbus TCP Config - V1 - 2Document27 pagesCustom Modbus TCP Config - V1 - 2Humberto BalderasNo ratings yet
- MGE UPS Systems EPS 6000 User Manual PDFDocument84 pagesMGE UPS Systems EPS 6000 User Manual PDFlyax1365No ratings yet
- GFK1645L VersaMax Miano Users ManualDocument733 pagesGFK1645L VersaMax Miano Users ManualAntonio ChoquevilcaNo ratings yet
- SYNC - DNP3 Slave Interface User Manual - Rev1.0.2 - ModDocument34 pagesSYNC - DNP3 Slave Interface User Manual - Rev1.0.2 - ModsyclonNo ratings yet
- ATV6000 Handbook Manual EN QGH83255 02.1Document226 pagesATV6000 Handbook Manual EN QGH83255 02.1nto_ntoNo ratings yet
- BAT - Operation and Maintenance Manual Rev2.5Document123 pagesBAT - Operation and Maintenance Manual Rev2.5Truong Hung50% (2)
- En - ku990r Svc Eng - 080611 Не Нужные Водяные ЗнакиDocument225 pagesEn - ku990r Svc Eng - 080611 Не Нужные Водяные ЗнакиMaxAllgeruNo ratings yet
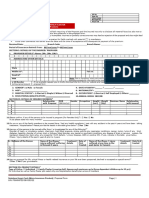
- Portability FormDocument2 pagesPortability FormFarshid BokdawallaNo ratings yet
- Portability Form Annexure 31-01-2012Document3 pagesPortability Form Annexure 31-01-2012irshadgraymanNo ratings yet
- Health InsuranceDocument18 pagesHealth Insurancesneha sarodeNo ratings yet
- Ihp FHP PF - 2023Document8 pagesIhp FHP PF - 2023Mantra ServicesNo ratings yet
- PP CformDocument4 pagesPP CformHihiNo ratings yet
- Sukshma Hospi CashDocument4 pagesSukshma Hospi CashAdemuyiwa OlaniyiNo ratings yet
- Revit 2010 ESPAÑOLDocument380 pagesRevit 2010 ESPAÑOLEmilio Castañon50% (2)
- Gapped SentencesDocument8 pagesGapped SentencesKianujillaNo ratings yet
- Big Joe Pds30-40Document198 pagesBig Joe Pds30-40mauro garciaNo ratings yet
- Essential Rendering BookDocument314 pagesEssential Rendering BookHelton OliveiraNo ratings yet
- Guia de Usuario GPS Spectra SP80 PDFDocument118 pagesGuia de Usuario GPS Spectra SP80 PDFAlbrichs BennettNo ratings yet
- Unit 14 Ergonomics Design: AND ProductDocument24 pagesUnit 14 Ergonomics Design: AND ProductRämêşh KątúřiNo ratings yet
- Easa Management System Assessment ToolDocument40 pagesEasa Management System Assessment ToolAdam Tudor-danielNo ratings yet
- Oxygen Cost and Energy Expenditure of RunningDocument7 pagesOxygen Cost and Energy Expenditure of Runningnb22714No ratings yet
- Joining Instruction 4 Years 22 23Document11 pagesJoining Instruction 4 Years 22 23Salmini ShamteNo ratings yet
- Peran Dan Tugas Receptionist Pada Pt. Serim Indonesia: Disadur Oleh: Dra. Nani Nuraini Sarah MsiDocument19 pagesPeran Dan Tugas Receptionist Pada Pt. Serim Indonesia: Disadur Oleh: Dra. Nani Nuraini Sarah MsiCynthia HtbNo ratings yet
- Listening Exercise 1Document1 pageListening Exercise 1Ma. Luiggie Teresita PerezNo ratings yet
- Typical T Intersection On Rural Local Road With Left Turn LanesDocument1 pageTypical T Intersection On Rural Local Road With Left Turn Lanesahmed.almakawyNo ratings yet
- LEARNING ACTIVITY Sheet Math 7 q3 M 1Document4 pagesLEARNING ACTIVITY Sheet Math 7 q3 M 1Mariel PastoleroNo ratings yet
- Technical Manual - C&C08 Digital Switching System Chapter 2 OverviewDocument19 pagesTechnical Manual - C&C08 Digital Switching System Chapter 2 OverviewSamuel100% (2)
- HP HP3-X11 Exam: A Composite Solution With Just One ClickDocument17 pagesHP HP3-X11 Exam: A Composite Solution With Just One ClicksunnyNo ratings yet
- Role of PAODocument29 pagesRole of PAOAjay DhokeNo ratings yet
- Copula and Multivariate Dependencies: Eric MarsdenDocument48 pagesCopula and Multivariate Dependencies: Eric MarsdenJeampierr Jiménez CheroNo ratings yet
- PEDs and InterferenceDocument28 pagesPEDs and Interferencezakool21No ratings yet
- Shopping Mall: Computer Application - IiiDocument15 pagesShopping Mall: Computer Application - IiiShadowdare VirkNo ratings yet
- BIT 4107 Mobile Application DevelopmentDocument136 pagesBIT 4107 Mobile Application DevelopmentVictor NyanumbaNo ratings yet
- 2021 JHS INSET Template For Modular/Online Learning: Curriculum MapDocument15 pages2021 JHS INSET Template For Modular/Online Learning: Curriculum MapDremie WorksNo ratings yet
- Paradigms of ManagementDocument2 pagesParadigms of ManagementLaura TicoiuNo ratings yet