You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Emcee Script For Hari Raya EventDocument2 pagesEmcee Script For Hari Raya Eventkylin kho100% (1)
- Fallen Angel Chapter OneDocument19 pagesFallen Angel Chapter OneDez Donaire100% (1)
- Regulatory Framework For Investment Banking in IndiaDocument2 pagesRegulatory Framework For Investment Banking in IndiaDevanshee Kothari0% (1)
- Generational CursesDocument5 pagesGenerational Cursesfatima110No ratings yet
- The True, Real, and Public Woman Portrayed in Ruth HallDocument16 pagesThe True, Real, and Public Woman Portrayed in Ruth HallElizabethNo ratings yet
- Lawsuit Against The LDS ChurchDocument38 pagesLawsuit Against The LDS ChurchThe Salt Lake TribuneNo ratings yet
- Contract of Lease-Water Refilling StationDocument4 pagesContract of Lease-Water Refilling StationEkeena Lim100% (1)
- Reproductions Supplied by EDRS Are The Best That Can Be Made From The Original DocumentDocument16 pagesReproductions Supplied by EDRS Are The Best That Can Be Made From The Original DocumentMaria MariaNo ratings yet
- Ida Report No 64 (Chest. KSP)Document72 pagesIda Report No 64 (Chest. KSP)Maria MariaNo ratings yet
- Bucuresti ComertDocument87 pagesBucuresti ComertEXDE601E100% (3)
- Art. - Qual - of Life AsthmaDocument6 pagesArt. - Qual - of Life AsthmaMaria MariaNo ratings yet
- E-Learning,, ,: Key WordsDocument8 pagesE-Learning,, ,: Key WordsMaria MariaNo ratings yet
- Intolerance of Uncertainty Moderates Anxiety (2010)Document5 pagesIntolerance of Uncertainty Moderates Anxiety (2010)Maria MariaNo ratings yet
- 2005meetingabstracts PDFDocument122 pages2005meetingabstracts PDFMaria MariaNo ratings yet
- Zinnbauer PargamentDocument21 pagesZinnbauer PargamentMaria MariaNo ratings yet
- Circulation 1979 Aronow 344 50Document8 pagesCirculation 1979 Aronow 344 50Maria MariaNo ratings yet
- 2005 Meeting AbstractsDocument122 pages2005 Meeting AbstractsMaria MariaNo ratings yet
- Civil Procedure - Seminar SixDocument25 pagesCivil Procedure - Seminar SixGrace YuNo ratings yet
- RIZAL Sa DAPITANDocument5 pagesRIZAL Sa DAPITANIra270% (1)
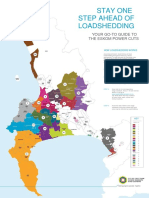
- Load Shedding All Areas Schedule and MapDocument2 pagesLoad Shedding All Areas Schedule and MapRobin VisserNo ratings yet
- People Vs Arnulfo FernandezDocument1 pagePeople Vs Arnulfo FernandezCharles Roger Raya100% (1)
- Digest PeopleVsHassanDocument2 pagesDigest PeopleVsHassanJappy Alon100% (1)
- G.R No. 173252 July 17, 2009 DIGESTDocument2 pagesG.R No. 173252 July 17, 2009 DIGESTChristine Jane Rodriguez100% (1)
- Semana 08 - InglesDocument6 pagesSemana 08 - InglesJulio Alberto Salcedo ParcoNo ratings yet
- Plan of DissertationDocument27 pagesPlan of DissertationPriya PuriNo ratings yet
- Operation Urgent FuryDocument40 pagesOperation Urgent FurygtrazorNo ratings yet
- Politicka Misao 1 2011 94 107 PDFDocument14 pagesPoliticka Misao 1 2011 94 107 PDFmilan trifunovicNo ratings yet
- The Monthly Hindu Review - Current Affairs - March 2023: WWW - Careerpower.in Adda247 AppDocument47 pagesThe Monthly Hindu Review - Current Affairs - March 2023: WWW - Careerpower.in Adda247 ApphhhNo ratings yet
- SK Internal Rules of Procedures, SkchairgpadiatonDocument12 pagesSK Internal Rules of Procedures, SkchairgpadiatonGp Marshall Adiaton75% (4)
- SimmonsDocument5 pagesSimmonshgkjgkg hkhNo ratings yet
- INVOICEDocument2 pagesINVOICEdiana rodreguzeNo ratings yet
- Case For TortsDocument34 pagesCase For Tortsadonis.orillaNo ratings yet
- Compassionate Communication and Empathy's Awakening Booklet - Nonviolent CommunicationDocument10 pagesCompassionate Communication and Empathy's Awakening Booklet - Nonviolent CommunicationNonViolent Communication100% (2)
- Sindh Land Revenue Act 1967Document62 pagesSindh Land Revenue Act 1967Tarique Jamali100% (1)
- Booking Confirmed: Flight Selection Passenger Information Additional Services PaymentDocument2 pagesBooking Confirmed: Flight Selection Passenger Information Additional Services PaymentMuhammad Usman BaigNo ratings yet
- Complete The Following Text With Words From The BoxDocument3 pagesComplete The Following Text With Words From The BoxMarques Picial JuniorNo ratings yet
- 20mm PGU-28 A/B SAPHEIDocument1 page20mm PGU-28 A/B SAPHEIMF84100% (1)
- Case # 13 - Mandatory - Ngo Yao Tit and Chua Eng Cheng vs. Sheriff of Manila, 27 Phil. 378Document2 pagesCase # 13 - Mandatory - Ngo Yao Tit and Chua Eng Cheng vs. Sheriff of Manila, 27 Phil. 378Julie RoldanNo ratings yet
- Cover PageDocument50 pagesCover Pagetavish koulNo ratings yet
- Human Rights - 2nd Sem 2k18-2k19 (Midterm)Document3 pagesHuman Rights - 2nd Sem 2k18-2k19 (Midterm)Jodi Anne AmoyoNo ratings yet