You might also like
- Surgical Endoscopy Aug1998Document99 pagesSurgical Endoscopy Aug1998Saibo BoldsaikhanNo ratings yet
- Endometrial Polyps With Open-Cervix Pyometra in A CatDocument4 pagesEndometrial Polyps With Open-Cervix Pyometra in A CatFajarAriefSumarnoNo ratings yet
- Javma 237 3 299Document5 pagesJavma 237 3 299tcvhNo ratings yet
- LeíomaDocument6 pagesLeíomaStephanie OdriozolaNo ratings yet
- Artigo 5Document8 pagesArtigo 5doctorbanNo ratings yet
- Single Incision, Laparoscopic-Assisted Ovariohysterectomy For Mucometra and Pyometra in DogsDocument5 pagesSingle Incision, Laparoscopic-Assisted Ovariohysterectomy For Mucometra and Pyometra in Dogsalfi fadilah alfidruNo ratings yet
- Tema 4 - Artículo 1 - Santl 1998Document12 pagesTema 4 - Artículo 1 - Santl 1998Nieves Anais Bustinza PahuaraNo ratings yet
- Hysterotomy of A Dairy Coe With Long-Time Macerated FoetusDocument10 pagesHysterotomy of A Dairy Coe With Long-Time Macerated FoetusmohammedNo ratings yet
- Bilateral Hydronephrosis and Hydroureter After Ovariohysterectomy Using Nylon Cable Tie: A Case ReportDocument5 pagesBilateral Hydronephrosis and Hydroureter After Ovariohysterectomy Using Nylon Cable Tie: A Case ReportReiner Silveira de MoraesNo ratings yet
- WWW - Vet 201508 0008Document4 pagesWWW - Vet 201508 0008Preston BoasythongNo ratings yet
- Surgical Management of An Abdominal Abscess in A Malayan TapirDocument3 pagesSurgical Management of An Abdominal Abscess in A Malayan TapirPaulo MorgadoNo ratings yet
- AsmaaDocument9 pagesAsmaaاسماء زياد عبدالجبارNo ratings yet
- Hyperoestrogenism and Mammary Adenosis Associated With A Metastatic Sertoli Cell Tumour in A Male Pekingese DogDocument5 pagesHyperoestrogenism and Mammary Adenosis Associated With A Metastatic Sertoli Cell Tumour in A Male Pekingese DogALAN RODRIGO ROJAS COVARRUBIASNo ratings yet
- Javma-Javma 258 1 85Document4 pagesJavma-Javma 258 1 85Carlos Rubiños AlonsoNo ratings yet
- Pyometra in A Cat: A Clinical Case Report: Research ArticleDocument6 pagesPyometra in A Cat: A Clinical Case Report: Research ArticleFajarAriefSumarnoNo ratings yet
- Z - 2001-01 - Nonfunctioning Islet Cell Carcinoma of The Pancreas Associated With Massive Intra-Abdominal HemorrhageDocument5 pagesZ - 2001-01 - Nonfunctioning Islet Cell Carcinoma of The Pancreas Associated With Massive Intra-Abdominal HemorrhageNawzad SulayvaniNo ratings yet
- ABRAVAS 5 de 9 - Hernandez Divers 2007 Liver BXDocument5 pagesABRAVAS 5 de 9 - Hernandez Divers 2007 Liver BXCamilo SantanderNo ratings yet
- Laparoscopic Colopexy in Dogs: Full Paper SurgeryDocument6 pagesLaparoscopic Colopexy in Dogs: Full Paper SurgeryrianperoNo ratings yet
- A Gigantic Ovarian Cyst A Case StudyDocument5 pagesA Gigantic Ovarian Cyst A Case Studyshaimaanassr25No ratings yet
- Treatmen 3Document6 pagesTreatmen 3Livia GudacNo ratings yet
- Urethral Advancement For Prox. HypospadiasDocument4 pagesUrethral Advancement For Prox. HypospadiasIoannis ValioulisNo ratings yet
- Atresia Ani Associated With Recto-Vaginal Fistula in Two Months Old Sudanesse Crossbreed LambDocument4 pagesAtresia Ani Associated With Recto-Vaginal Fistula in Two Months Old Sudanesse Crossbreed LambPanjul NugrohoNo ratings yet
- Laparoscopic Management of Giant Ovarian Cyst A Case ReportDocument3 pagesLaparoscopic Management of Giant Ovarian Cyst A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Generalized Calcinosis Cutis Associated With Probable Leptospirosis in A Dog (Pages 401-406)Document6 pagesGeneralized Calcinosis Cutis Associated With Probable Leptospirosis in A Dog (Pages 401-406)jenNo ratings yet
- Priapism Secondary To Perineal Abscess in A Dog - A Case Report.Document7 pagesPriapism Secondary To Perineal Abscess in A Dog - A Case Report.Mauricio MorilloNo ratings yet
- Guthrie2014 PubmedDocument5 pagesGuthrie2014 Pubmedtycia.vilelaNo ratings yet
- Case Report Diastasis PubisDocument11 pagesCase Report Diastasis Pubistresna anggaNo ratings yet
- Laparoscopic Orchidopexy: Current Surgical Opinion.: AbstractDocument6 pagesLaparoscopic Orchidopexy: Current Surgical Opinion.: AbstractGemiNo ratings yet
- Bazo Errante 2016 REVISED Ijtra1601084Document4 pagesBazo Errante 2016 REVISED Ijtra1601084luisalfredo_montesNo ratings yet
- 2019 RMC1Document16 pages2019 RMC1corinaNo ratings yet
- Case Study Mastectomy RevisedDocument13 pagesCase Study Mastectomy RevisedJessa BorreNo ratings yet
- Cistectomia Radical Art08 PDFDocument7 pagesCistectomia Radical Art08 PDFJoshua GardnerNo ratings yet
- Canine Lipomas Treated With Steroid InjectionsDocument5 pagesCanine Lipomas Treated With Steroid InjectionsAnonymous mwZjiriNo ratings yet
- Meigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsDocument6 pagesMeigs' Syndrome and Pseudo-Meigs' Syndrome: Report of Four Cases and Literature ReviewsAlfa FebriandaNo ratings yet
- Nolff - Treatment of A Perforating Thoracic Bite Wound in A Dog With NPWTDocument7 pagesNolff - Treatment of A Perforating Thoracic Bite Wound in A Dog With NPWTOliviaQFNo ratings yet
- A Case of Transmissible Venereal Tumor in A Castrated Dog in Benue State, NigeriaDocument4 pagesA Case of Transmissible Venereal Tumor in A Castrated Dog in Benue State, NigeriaYuni SemidiNo ratings yet
- Tuberculosis of The Chest Wall With Massive Tuberculous Pleural EffusionDocument3 pagesTuberculosis of The Chest Wall With Massive Tuberculous Pleural EffusionwulanNo ratings yet
- Affections of The Salivary Ducts in Buffaloes: ISSN: 2226-4485 (Print) ISSN: 2218-6050 (Online)Document4 pagesAffections of The Salivary Ducts in Buffaloes: ISSN: 2226-4485 (Print) ISSN: 2218-6050 (Online)TriandNo ratings yet
- Laparoscopic Ovariectomy in Standing Donkeys by Using A New InstrumentDocument8 pagesLaparoscopic Ovariectomy in Standing Donkeys by Using A New InstrumentWahyu Dwi NugrohoNo ratings yet
- Journal 2015Document3 pagesJournal 2015Rakha Sulthan SalimNo ratings yet
- Pancreas FelinoDocument7 pagesPancreas FelinoLorena Millan VarelaNo ratings yet
- Hypospadias: by Khaled Ashour John Radcliffe HsopitalDocument87 pagesHypospadias: by Khaled Ashour John Radcliffe Hsopitalhayssam rashwanNo ratings yet
- Infected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantDocument4 pagesInfected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantIJAR JOURNALNo ratings yet
- Case Series of Unusual Causes Intestinal Obstruction in Infants and ChildrenDocument9 pagesCase Series of Unusual Causes Intestinal Obstruction in Infants and ChildrenSnega KaranNo ratings yet
- Diagnostic Tools in ObgynDocument27 pagesDiagnostic Tools in ObgynHenok Y KebedeNo ratings yet
- Case Presentation: Presenter Dejene (GSR)Document14 pagesCase Presentation: Presenter Dejene (GSR)Dajanee Ittaanaa DhaabaaNo ratings yet
- Ectopic Abdominal Pregnancies: About 2 CasesDocument10 pagesEctopic Abdominal Pregnancies: About 2 CasesIJAR JOURNALNo ratings yet
- Ureteral ReconstructionDocument6 pagesUreteral ReconstructiongumNo ratings yet
- Congenital Hyperinsulinism of The Newborn: A Case ReportDocument6 pagesCongenital Hyperinsulinism of The Newborn: A Case ReportEdi SetiawanNo ratings yet
- Research Article: Isolated Male Epispadias: Anatomic Functional Restoration Is The Primary GoalDocument4 pagesResearch Article: Isolated Male Epispadias: Anatomic Functional Restoration Is The Primary GoalsatriamarrantizaNo ratings yet
- Dandy Hollow Organ PerforationDocument13 pagesDandy Hollow Organ PerforationyongkyNo ratings yet
- Congenital Urachal Diverticulum in Dogs: A Case Report: Ojszczyk-Szczepaniak A., Miech A., Wojnowski TDocument4 pagesCongenital Urachal Diverticulum in Dogs: A Case Report: Ojszczyk-Szczepaniak A., Miech A., Wojnowski TMarina MagalhãesNo ratings yet
- Ultrasonography of The Bovine Udder PDFDocument17 pagesUltrasonography of The Bovine Udder PDFCarla Meza OrtizNo ratings yet
- Case Report HisprungDocument11 pagesCase Report HisprungAnggun Dwi Jayanti0% (1)
- Surgical Treatment of Displaced Abomasum in Cattle Using Ljubljana MethodDocument8 pagesSurgical Treatment of Displaced Abomasum in Cattle Using Ljubljana MethodIkhwanul KhairiaNo ratings yet
- Cap Polyposis in Children: Case Report and Literature ReviewDocument6 pagesCap Polyposis in Children: Case Report and Literature ReviewLuis ArrietaNo ratings yet
- Total Abdominal Hysterectomy Bilateral Salpingo OophorectomyDocument3 pagesTotal Abdominal Hysterectomy Bilateral Salpingo OophorectomyLouise Bravo100% (1)
- Undescended TestisDocument3 pagesUndescended TestisIoannis ValioulisNo ratings yet
- 2019 Simplified Minimally Invasive Surgical Approach For Prophylactic Laparoscopic Gastropexy in 21 CasesDocument8 pages2019 Simplified Minimally Invasive Surgical Approach For Prophylactic Laparoscopic Gastropexy in 21 CasesrizalakbarsyaNo ratings yet
- No Hewan Grooming Biasa Jamur Kutu Jamur+KutuDocument2 pagesNo Hewan Grooming Biasa Jamur Kutu Jamur+KutuTia KawairiIzhukaNo ratings yet
- Cats. ++++Document1 pageCats. ++++Tia KawairiIzhukaNo ratings yet
- Toxocariasis: Asymptomatic So They Can Not Detected. BlindnessDocument1 pageToxocariasis: Asymptomatic So They Can Not Detected. BlindnessTia KawairiIzhukaNo ratings yet
- Dwi Mutiara Sari - 2013a - 135130101111018Document3 pagesDwi Mutiara Sari - 2013a - 135130101111018Tia KawairiIzhukaNo ratings yet
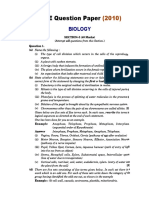
- ICSE QUESTION PAPER Biology 2010 Class 10 PDFDocument11 pagesICSE QUESTION PAPER Biology 2010 Class 10 PDFLokesh MalikNo ratings yet
- Скелетна ммускулна клетка - устройство на саркомерDocument4 pagesСкелетна ммускулна клетка - устройство на саркомерMartin PetkovNo ratings yet
- Grade 9 ScienceDocument19 pagesGrade 9 ScienceChristine Grace GiradoNo ratings yet
- Gram Staining Protocol or ProcedureDocument4 pagesGram Staining Protocol or Procedurearavindbt2523No ratings yet
- BILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationDocument1 pageBILAL FARID, 1 Year(s) /male: Registration Date: M.R. No: Registration At: Sample LocationsaifNo ratings yet
- Appearances - How To Describe Someone in EnglishDocument26 pagesAppearances - How To Describe Someone in EnglishNadia Tara DilaNo ratings yet
- 6 1 1 Student ResponseDocument10 pages6 1 1 Student Responseapi-255602834No ratings yet
- Respiratory Physiology: Control of The Upper Airway: Richard L. Horner University of TorontoDocument8 pagesRespiratory Physiology: Control of The Upper Airway: Richard L. Horner University of TorontoDopamina PsicoactivaNo ratings yet
- Chap 8Document17 pagesChap 8Shane EsparasNo ratings yet
- Hormones and The Endocrine System - Johns Hopkins MedicineDocument5 pagesHormones and The Endocrine System - Johns Hopkins MedicineAnjaliNo ratings yet
- Blood Group & RHDocument27 pagesBlood Group & RHfamtaluNo ratings yet
- MVW 020Document9 pagesMVW 020SofyanNo ratings yet
- DLP VALDERAMA Carla Ann - BSE SCIENCE IV DEMODocument19 pagesDLP VALDERAMA Carla Ann - BSE SCIENCE IV DEMOMarvi ValdezNo ratings yet
- Embryology Testis 08 PDFDocument20 pagesEmbryology Testis 08 PDFNanang Abdul AzizNo ratings yet
- English For MedicineDocument52 pagesEnglish For MedicineRoya NaderiNo ratings yet
- Embriologi Tumbuhan - Materi 2Document21 pagesEmbriologi Tumbuhan - Materi 2gahanNo ratings yet
- Anatomy of A Frog ReadingDocument3 pagesAnatomy of A Frog ReadingRyan Carlo CondeNo ratings yet
- Anatomy AND Physiology: The Human As An OrganismsDocument26 pagesAnatomy AND Physiology: The Human As An OrganismsJake Donely C. PaduaNo ratings yet
- List of Surgical ProceduresDocument3 pagesList of Surgical ProceduresAtto AmpereNo ratings yet
- Reproductive SystemDocument49 pagesReproductive SystemAyro Business CenterNo ratings yet
- 2021 ESC Preporuke Za Srčani Pejsing I Srčanu Resinhronizacionu TerapijuDocument68 pages2021 ESC Preporuke Za Srčani Pejsing I Srčanu Resinhronizacionu TerapijuDaria Lily MićanovićNo ratings yet
- Unit 1 Anatomy, Physiology and The Human Body: Learning OutcomesDocument91 pagesUnit 1 Anatomy, Physiology and The Human Body: Learning OutcomesDeolita BadiangNo ratings yet
- KP 2. Pengaruh Agen Biologi Dan Mekanisme Perubahan Sel Serta Penyakit Yang DitimbulkannyaDocument28 pagesKP 2. Pengaruh Agen Biologi Dan Mekanisme Perubahan Sel Serta Penyakit Yang DitimbulkannyaShintia Surya PutriNo ratings yet
- Caiet de SarciniDocument33 pagesCaiet de SarciniEta TrutaNo ratings yet
- Hemorrhagic Conditions of Late Pregnancy Other Related Problems 1Document5 pagesHemorrhagic Conditions of Late Pregnancy Other Related Problems 1imnasNo ratings yet
- Cord Pulmonar CronicDocument11 pagesCord Pulmonar CronicroxanachiticNo ratings yet
- Nephrotic SyndromeDocument38 pagesNephrotic SyndromeSwati SharmaNo ratings yet
- Kuliah Biokimia-Imunokimia FK UNDIPDocument19 pagesKuliah Biokimia-Imunokimia FK UNDIPPutri HapsariNo ratings yet
- Effects of Myofascial Release and Stretching Technique On ROM and Reaction Time PDFDocument3 pagesEffects of Myofascial Release and Stretching Technique On ROM and Reaction Time PDFfisionovaisNo ratings yet