You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ACLS Full Lesson Plans PDFDocument60 pagesACLS Full Lesson Plans PDFVictoriano Mendez100% (1)
- Health According To The Scriptures - Paul NisonDocument306 pagesHealth According To The Scriptures - Paul NisonJSonJudah100% (1)
- Primary Health Care Hand Outs For StudentsDocument35 pagesPrimary Health Care Hand Outs For Studentsyabaeve100% (6)
- Neurology - Anatomy Stuff UAWDocument329 pagesNeurology - Anatomy Stuff UAWNabeel Shahzad100% (1)
- ATTinchronicliverdisease JCEH2012Document12 pagesATTinchronicliverdisease JCEH2012Anonymous 1EQutBNo ratings yet
- Oce Guera 2016Document6 pagesOce Guera 2016Anonymous 1EQutBNo ratings yet
- Cirrosis Hepatica DescompensadaDocument55 pagesCirrosis Hepatica DescompensadaJefferson Diaz100% (1)
- TB Hivmodule23.05.07Document104 pagesTB Hivmodule23.05.07Pratiwi TiwiNo ratings yet
- Bmri2019 3951574Document10 pagesBmri2019 3951574Anonymous 1EQutBNo ratings yet
- Tahara2008 Article AbnormalGrowthFactorCytokineNeDocument7 pagesTahara2008 Article AbnormalGrowthFactorCytokineNeAnonymous 1EQutBNo ratings yet
- Jadwal Workshop Dan Simposium M7, 22 Jan 2020Document7 pagesJadwal Workshop Dan Simposium M7, 22 Jan 2020Anonymous 1EQutBNo ratings yet
- Gastrin and Gastric CancerDocument9 pagesGastrin and Gastric CancerlannaNo ratings yet
- Archives of Gastroenterological Case ReportsDocument2 pagesArchives of Gastroenterological Case ReportsAnonymous 1EQutBNo ratings yet
- P. Tonino - Gastritis and Gastric Cancer - New Insights in Gastroprot., Diag.,Trtmts (2011, Intech)Document308 pagesP. Tonino - Gastritis and Gastric Cancer - New Insights in Gastroprot., Diag.,Trtmts (2011, Intech)Anonymous 1EQutBNo ratings yet
- Glycemic Control and Rate of Sputum Conversion in Diabetic Patients With Pulmonary Tuberculosis LDT 1000104Document3 pagesGlycemic Control and Rate of Sputum Conversion in Diabetic Patients With Pulmonary Tuberculosis LDT 1000104Anonymous 1EQutBNo ratings yet
- Glycemic Control and Rate of Sputum Conversion in Diabetic Patients With Pulmonary Tuberculosis LDT 1000104Document3 pagesGlycemic Control and Rate of Sputum Conversion in Diabetic Patients With Pulmonary Tuberculosis LDT 1000104Anonymous 1EQutBNo ratings yet
- Gastrin and Gastric CancerDocument9 pagesGastrin and Gastric CancerlannaNo ratings yet
- Ni Hms 585691Document20 pagesNi Hms 585691Anonymous 1EQutBNo ratings yet
- Chapter 2Document34 pagesChapter 2Anonymous 1EQutBNo ratings yet
- Peritoneal Dialysis Versus Hemodialysis: Risks, Benefits, and Access IssuesDocument5 pagesPeritoneal Dialysis Versus Hemodialysis: Risks, Benefits, and Access IssuesAnonymous 1EQutBNo ratings yet
- J Small Anim Pract 2007 - Effects of Postoperative Ketamine Infusion On Pain Control and Feeding Behaviour in Bitches Unedrgoing MastectomyDocument8 pagesJ Small Anim Pract 2007 - Effects of Postoperative Ketamine Infusion On Pain Control and Feeding Behaviour in Bitches Unedrgoing MastectomyAnonymous 1EQutBNo ratings yet
- Hepatitis B and HIV CoinfectionDocument9 pagesHepatitis B and HIV CoinfectionAnonymous 1EQutBNo ratings yet
- Monta Ez Barra GN 2014Document11 pagesMonta Ez Barra GN 2014Anonymous 1EQutBNo ratings yet
- Mart N Calder N 2015Document5 pagesMart N Calder N 2015Anonymous 1EQutBNo ratings yet
- Analgesia ProtocolDocument4 pagesAnalgesia ProtocolAnonymous 1EQutBNo ratings yet
- Dapus SsDocument3 pagesDapus SsAnonymous 1EQutBNo ratings yet
- Chapter 5 Glucose HomeostasisDocument15 pagesChapter 5 Glucose Homeostasistliviu334066No ratings yet
- Hyper Guidelines 2011Document65 pagesHyper Guidelines 2011wrocha2000No ratings yet
- Anaesthetic Considerations in Cardiac PatientsDocument7 pagesAnaesthetic Considerations in Cardiac PatientsAnonymous 1EQutBNo ratings yet
- Jpga 61 248Document5 pagesJpga 61 248Anonymous 1EQutBNo ratings yet
- Undangan KesitDocument1 pageUndangan KesitAnonymous 1EQutBNo ratings yet
- IndianJAnaesth60119-3742867 102348Document6 pagesIndianJAnaesth60119-3742867 102348Anonymous 1EQutBNo ratings yet
- IndianJAnaesth599542-3768369 102803Document8 pagesIndianJAnaesth599542-3768369 102803Anonymous 1EQutBNo ratings yet
- Clinico-Pathological Study On Haemophilia: An Analysis of 50 CasesDocument4 pagesClinico-Pathological Study On Haemophilia: An Analysis of 50 CasesSajjad Hossain ShuvoNo ratings yet
- BehandlungskarteiDocument2 pagesBehandlungskarteidenyse bakkerNo ratings yet
- Understanding Cancer Treatment and OutcomesDocument5 pagesUnderstanding Cancer Treatment and OutcomesMr. questionNo ratings yet
- Adrenal Function Urine TestDocument30 pagesAdrenal Function Urine TestDamarys ReyesNo ratings yet
- Deenanath Mangeshkar HospitalDocument11 pagesDeenanath Mangeshkar HospitalIti GoyalNo ratings yet
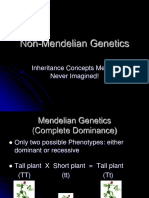
- Non-Mendelian Inheritance2Document41 pagesNon-Mendelian Inheritance2Jeremy Christian MendozaNo ratings yet
- Phalaenopsis ManualDocument11 pagesPhalaenopsis ManualChanaka MallikarachchiNo ratings yet
- Practice Exam QuestionsDocument8 pagesPractice Exam QuestionsHari Babu25% (4)
- Kidney CancerDocument6 pagesKidney CancerAKHILNo ratings yet
- Jurnal GerdDocument6 pagesJurnal GerddilaNo ratings yet
- Infection Control Committee 6 Icc. Meeting DATE: MAY 22, 2020 TIME: 11:50 AM - 3:40 PM Venue: Board Room, Administrative Office 10Th FloorDocument7 pagesInfection Control Committee 6 Icc. Meeting DATE: MAY 22, 2020 TIME: 11:50 AM - 3:40 PM Venue: Board Room, Administrative Office 10Th FloorCris GalendezNo ratings yet
- Python Ieee Projects 2021 - 22 JPDocument3 pagesPython Ieee Projects 2021 - 22 JPWebsoft Tech-HydNo ratings yet
- Biological Factors Responsible For Failure of Osseointegration in OralimplantsDocument7 pagesBiological Factors Responsible For Failure of Osseointegration in OralimplantsKarim MohamedNo ratings yet
- Return Permit For Resident Outside UAEDocument3 pagesReturn Permit For Resident Outside UAElloyd kampunga100% (1)
- Reader S Digest Asia English Edition - December 2023january 2024Document116 pagesReader S Digest Asia English Edition - December 2023january 2024Kriangyut WorrasritakankulNo ratings yet
- Pioped PDFDocument7 pagesPioped PDFaiNo ratings yet
- Drug InteractionsDocument11 pagesDrug InteractionssamNo ratings yet
- HCM Treatment Italy Ammirati2016Document13 pagesHCM Treatment Italy Ammirati2016xy manNo ratings yet
- Presentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONDocument23 pagesPresentation On Hysterosalpingography: BY Mahmud M Alkali I.D: 12/01/09/069 Radiography, Unimaid. 2014/2015 SESSIONMubarak M AlkaliNo ratings yet
- Anger: Realized By: Supervised byDocument15 pagesAnger: Realized By: Supervised byChahinaz Frid-ZahraouiNo ratings yet
- Premio 20 DTDocument35 pagesPremio 20 DThyakueNo ratings yet
- Crim 2 Assignment Title 8 of RPC Book 2Document8 pagesCrim 2 Assignment Title 8 of RPC Book 2Gio AvilaNo ratings yet
- Fact Sheet YaconDocument2 pagesFact Sheet YaconTrilceNo ratings yet
- COVID 19 Guideline To Resume Paediatric Dental Services in MalaysiaDocument29 pagesCOVID 19 Guideline To Resume Paediatric Dental Services in MalaysiaEnrita DianNo ratings yet
- History of Nursing and The Development of The ProfessionDocument4 pagesHistory of Nursing and The Development of The Professionastraia celesteNo ratings yet
- Big Data Final ReportDocument34 pagesBig Data Final Reportclinfox100% (2)