You might also like
- Inflammation NotesDocument47 pagesInflammation Notespuji100% (2)
- InflammationDocument48 pagesInflammationTewodros TeshomeNo ratings yet
- Paper 2Document71 pagesPaper 2Edward AngimoyNo ratings yet
- CPAT3201 2020 Inflammation Lecture 1 NOTESDocument50 pagesCPAT3201 2020 Inflammation Lecture 1 NOTESJoshua KaoNo ratings yet
- Chapter 2 Inflamation (B)Document86 pagesChapter 2 Inflamation (B)مختبرات ابوسارةNo ratings yet
- InflammationDocument8 pagesInflammationGhazi Uddin AhmedNo ratings yet
- Mechanisms of Inflammation I, II, and III LOsDocument9 pagesMechanisms of Inflammation I, II, and III LOsAndrew SagalovNo ratings yet
- Inflammation: Department of Pathology Anatomy Faculty of Medicine GMUDocument87 pagesInflammation: Department of Pathology Anatomy Faculty of Medicine GMUjeinpratpongNo ratings yet
- ACUTE INFLAMMATION VS CHRONIC INFLAMMATION Assignment #2 (CU-1774-2020)Document17 pagesACUTE INFLAMMATION VS CHRONIC INFLAMMATION Assignment #2 (CU-1774-2020)Ali Aasam KhanNo ratings yet
- 3.inflammation ProcessDocument13 pages3.inflammation ProcessGerald Limo Arap ChebiiNo ratings yet
- Mimiproject Anti InfiamationDocument69 pagesMimiproject Anti Infiamationmukeshcilaveni18No ratings yet
- 3.inflammation & Wound HealingDocument78 pages3.inflammation & Wound HealingEsaias ChanieNo ratings yet
- Inflammation & Repair Lecture (1) : Abuobaida E. E. AbukhelaifDocument15 pagesInflammation & Repair Lecture (1) : Abuobaida E. E. AbukhelaifSaboNo ratings yet
- Acute Inflammation PDFDocument6 pagesAcute Inflammation PDFHusseini ElghamryNo ratings yet
- Pathology (Inflammation and Wound Healing)Document14 pagesPathology (Inflammation and Wound Healing)andrew100% (1)
- Inflammation 30.08.2022Document39 pagesInflammation 30.08.2022Abdur RaquibNo ratings yet
- Acute InflammationDocument6 pagesAcute InflammationHusseini ElghamryNo ratings yet
- Acute InflammationDocument20 pagesAcute Inflammationbpt20% (2)
- Skenario IDocument12 pagesSkenario IRajasa FathahilllahNo ratings yet
- IVMS - General Pathology, Inflammation NotesDocument19 pagesIVMS - General Pathology, Inflammation NotesMarc Imhotep Cray, M.D.No ratings yet
- Inflammation: Course Teacher: Imon RahmanDocument21 pagesInflammation: Course Teacher: Imon RahmanDaksh SabharwalNo ratings yet
- Acute InflammationDocument76 pagesAcute InflammationOmor faruk HridoyNo ratings yet
- Acute and Chronic InflammationDocument13 pagesAcute and Chronic InflammationReymond MagnoNo ratings yet
- Cardinal Signs of InlamationDocument13 pagesCardinal Signs of InlamationKeshen KadumaNo ratings yet
- Inflammation NotesDocument12 pagesInflammation NotesavidadarkestevillearnNo ratings yet
- Unit 4.1Document8 pagesUnit 4.1Bloody MarieNo ratings yet
- Inflammation and RepairDocument2 pagesInflammation and RepairSha BtstaNo ratings yet
- Inflammation: Last Updated: April 6, 2022Document19 pagesInflammation: Last Updated: April 6, 2022Sopitha ThangamaniNo ratings yet
- InflammationDefinition, Symptoms, Treatment,&FactsBritannica 1710882912933Document6 pagesInflammationDefinition, Symptoms, Treatment,&FactsBritannica 1710882912933muhellen8No ratings yet
- Print Patho 1Document49 pagesPrint Patho 1insyiisyaNo ratings yet
- Caso ClinicoDocument30 pagesCaso ClinicoMINITZA MEDRANONo ratings yet
- Acute and Chronic Inflammation: Yacob Alemu (MD) May 2021Document89 pagesAcute and Chronic Inflammation: Yacob Alemu (MD) May 2021Tazeb AyeleNo ratings yet
- Inflammation Group. 1 PresentationDocument19 pagesInflammation Group. 1 PresentationMarry JuttNo ratings yet
- Inflamation: Drh. M. Arfan Lesmana, M.Sc. Fakultas Kedokteran Hewan, Universitas Brawijaya EmailDocument55 pagesInflamation: Drh. M. Arfan Lesmana, M.Sc. Fakultas Kedokteran Hewan, Universitas Brawijaya EmailalrezaNo ratings yet
- PHAR 233-InflammationDocument67 pagesPHAR 233-InflammationLina RamojNo ratings yet
- Inflammation and Tissue Repair: July 2021Document54 pagesInflammation and Tissue Repair: July 2021EdenNo ratings yet
- 04.inflammation 4-ChronicInflammationDocument34 pages04.inflammation 4-ChronicInflammationShameena KnNo ratings yet
- Module 3 InflammationDocument10 pagesModule 3 InflammationDanielle HayagNo ratings yet
- Inflammation 3Document44 pagesInflammation 3mikiyaskayleNo ratings yet
- Inflammation Is Part of The Complex Biological Response of Vascular Tissues To Harmful StimuliDocument2 pagesInflammation Is Part of The Complex Biological Response of Vascular Tissues To Harmful StimuliGabitza GabiNo ratings yet
- Inflammation and Inflammatory MediatorsDocument28 pagesInflammation and Inflammatory Mediatorsla.instagramawaNo ratings yet
- Lesi Rongga Mulut Diagnosis Dan Penanganannya PDFDocument35 pagesLesi Rongga Mulut Diagnosis Dan Penanganannya PDFFhaNo ratings yet
- 1 PATHO 2a - Inflammation - Dr. BailonDocument12 pages1 PATHO 2a - Inflammation - Dr. BailontonNo ratings yet
- Inflammation and RepairDocument21 pagesInflammation and RepairlolNo ratings yet
- Review Article: Role of Antioxidants and Natural Products in InflammationDocument15 pagesReview Article: Role of Antioxidants and Natural Products in InflammationMI SsouNo ratings yet
- Handouts - 6BIOM002W.2 - Inflammation 2018-9 PDFDocument66 pagesHandouts - 6BIOM002W.2 - Inflammation 2018-9 PDFFatima HusseinNo ratings yet
- Patho A 1. 3 Inflammation and Repair (Dy-Quiangco, 2015)Document13 pagesPatho A 1. 3 Inflammation and Repair (Dy-Quiangco, 2015)kristineNo ratings yet
- Inflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationDocument35 pagesInflammation and Repair: Definition of Inflammation Acute Inflammation Vascular Events in InflammationSoji AdimulaNo ratings yet
- لقطة شاشة ٢٠٢٣-١١-٠٩ في ٨.٥٣.٥٠ صDocument7 pagesلقطة شاشة ٢٠٢٣-١١-٠٩ في ٨.٥٣.٥٠ صmo44hh44No ratings yet
- Inflammation and RepairDocument5 pagesInflammation and RepairDENILLE AIRA NOGOYNo ratings yet
- Satria AdiDocument14 pagesSatria AdiSatria Adi PutraNo ratings yet
- Chronic InflammationDocument29 pagesChronic Inflammationparishaparisha433No ratings yet
- Adobe Scan 21 Jan 2024Document14 pagesAdobe Scan 21 Jan 2024pandapriyanka565No ratings yet
- 1.inflammation & Repair: Cardinal Signs of InflammationDocument47 pages1.inflammation & Repair: Cardinal Signs of Inflammationsharu4291No ratings yet
- A Inflammation For NursingDocument47 pagesA Inflammation For NursingSintayehu MulatuNo ratings yet
- Nursing:: CommunityDocument59 pagesNursing:: CommunityIlyes RaniNo ratings yet
- Inflammation and HealingDocument23 pagesInflammation and Healingatiqullah tarmiziNo ratings yet
- 7.2 Muscular System: Human Anatomy and Physiology With Pathophysiology LectureDocument3 pages7.2 Muscular System: Human Anatomy and Physiology With Pathophysiology LectureRamea LamanoNo ratings yet
- Sound or MantraDocument1 pageSound or MantrasureshbabubnysNo ratings yet
- Sunlight Therapy and EffectsDocument6 pagesSunlight Therapy and EffectssureshbabubnysNo ratings yet
- Tutorial 2, Plasma MembraneDocument51 pagesTutorial 2, Plasma MembranesureshbabubnysNo ratings yet
- Sudharsana KriyaDocument2 pagesSudharsana KriyasureshbabubnysNo ratings yet
- Nutritive Value of FoodDocument10 pagesNutritive Value of FoodsureshbabubnysNo ratings yet
- Suffocation and Artificial RespirationDocument3 pagesSuffocation and Artificial RespirationsureshbabubnysNo ratings yet
- First Aid InstructionDocument4 pagesFirst Aid InstructionsureshbabubnysNo ratings yet
- Sun and WaterDocument11 pagesSun and WatersureshbabubnysNo ratings yet
- CompressDocument3 pagesCompresssureshbabubnysNo ratings yet
- Laghu Shankha Prakshalana - Final BnysDocument9 pagesLaghu Shankha Prakshalana - Final Bnyssureshbabubnys100% (1)
- Properties of WaterDocument21 pagesProperties of WatersureshbabubnysNo ratings yet
- Sun Therapy For PsoriasisDocument11 pagesSun Therapy For PsoriasissureshbabubnysNo ratings yet
- ScienceDocument1 pageSciencesureshbabubnysNo ratings yet
- Effect of Chest PackDocument2 pagesEffect of Chest PacksureshbabubnysNo ratings yet
- Hospital ManagementDocument38 pagesHospital ManagementsureshbabubnysNo ratings yet
- Yoga For General PublicDocument25 pagesYoga For General PublicsureshbabubnysNo ratings yet
- DisasterDocument12 pagesDisastersureshbabubnysNo ratings yet
- Lipolysis LipogenesisDocument24 pagesLipolysis LipogenesissureshbabubnysNo ratings yet
- Fat Metabolism: I'm Not Fat, I've Just Got A Lot of Potential Energy!Document25 pagesFat Metabolism: I'm Not Fat, I've Just Got A Lot of Potential Energy!sureshbabubnysNo ratings yet
- HypothyroidismDocument7 pagesHypothyroidismsureshbabubnysNo ratings yet
- Con VacationDocument2 pagesCon VacationsureshbabubnysNo ratings yet
- Cardiac Rehabilitation CentreDocument7 pagesCardiac Rehabilitation CentresureshbabubnysNo ratings yet
- It Is Our Special Treatment Method in Which Kali MittiDocument3 pagesIt Is Our Special Treatment Method in Which Kali MittisureshbabubnysNo ratings yet
- Babu AstrologyDocument11 pagesBabu AstrologysureshbabubnysNo ratings yet
- Achampathu 1Document5 pagesAchampathu 1sureshbabubnysNo ratings yet
- GB and BB Training Agenda, Trainer and Certification Company ProfileDocument8 pagesGB and BB Training Agenda, Trainer and Certification Company ProfilesureshbabubnysNo ratings yet
- Dhirendra Brahmachari Sukshma Vyayama Subtle YogaDocument29 pagesDhirendra Brahmachari Sukshma Vyayama Subtle Yogadryashtokas93% (15)
- Meyyammal 44Document4 pagesMeyyammal 44sureshbabubnysNo ratings yet
- $ Mus KPF Fug GZRHKP - Jpug Ghiy - Kjiu: - YtndDocument5 pages$ Mus KPF Fug GZRHKP - Jpug Ghiy - Kjiu: - YtndsureshbabubnysNo ratings yet
- Chapter 8 WBCDocument39 pagesChapter 8 WBCMariel Lee ChingNo ratings yet
- (S.C. Rastogi) Essentials of Animal Physiology, 4t (BookSee - Org) 247Document1 page(S.C. Rastogi) Essentials of Animal Physiology, 4t (BookSee - Org) 247Indah Rizka AprilianiNo ratings yet
- Pathology NotesDocument29 pagesPathology NotesMK100% (1)
- Top 5 Leukogram Patterns Associated With Abnormal Neutrophil Concentrations CLDocument22 pagesTop 5 Leukogram Patterns Associated With Abnormal Neutrophil Concentrations CLXiuhuitzilli SanchezNo ratings yet
- Mechanism of Inflammation (DRG Hesti) PPTDocument27 pagesMechanism of Inflammation (DRG Hesti) PPTTifani Cita DewiNo ratings yet
- 17 Human Health and Disease: SolutionsDocument14 pages17 Human Health and Disease: SolutionsEkta ManglaniNo ratings yet
- 834-Article Text-2109-1-10-20210830Document8 pages834-Article Text-2109-1-10-20210830Vincentia Christinanda DonataNo ratings yet
- Ajplung 1993 265 3 l286Document7 pagesAjplung 1993 265 3 l286moussaouiNo ratings yet
- Correctly: IncorrectlyDocument70 pagesCorrectly: IncorrectlyDjdjjd Siisus100% (1)
- Cystic Fibrosis: Pathophysiology of Lung DiseaseDocument12 pagesCystic Fibrosis: Pathophysiology of Lung DiseaseGaby RojasNo ratings yet
- Hematology 425, LeukopoiesisDocument56 pagesHematology 425, LeukopoiesishanzukikNo ratings yet
- Soalan Objektif Bab 10 & Bab 11Document16 pagesSoalan Objektif Bab 10 & Bab 11Sains Matematik PahangNo ratings yet
- Inflammation and RepairDocument38 pagesInflammation and RepairIsaac Nsiah Acheampong100% (1)
- Ojsadmin, 1491Document4 pagesOjsadmin, 1491Cristian PeñaNo ratings yet
- Hydrogen PeroxideDocument85 pagesHydrogen PeroxideAnonymous yXCbTbHmh100% (2)
- Textbook of Diagnostic Microbiology 4th Edition Mahon Test BankDocument13 pagesTextbook of Diagnostic Microbiology 4th Edition Mahon Test Banklaylafarleyh3i8j9100% (26)
- Blood Anatomy and Physiology ReviewDocument20 pagesBlood Anatomy and Physiology ReviewStacey CamilleNo ratings yet
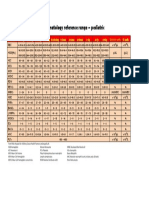
- Hematology Reference RangeDocument1 pageHematology Reference RangeNheeya WarzNo ratings yet
- Journal of Allergy and Clinical ImmunologyDocument265 pagesJournal of Allergy and Clinical Immunologydod_nurNo ratings yet
- Estafilococo Aureus Patogenicidad. Virulencia 2021Document23 pagesEstafilococo Aureus Patogenicidad. Virulencia 2021Gabriela ChaconNo ratings yet
- Neutrophil Extracellular Traps (Nets) - Formation and ImplicationsDocument9 pagesNeutrophil Extracellular Traps (Nets) - Formation and ImplicationsNurfitrianti ArfahNo ratings yet
- Hypersensitivity AssignmentDocument6 pagesHypersensitivity AssignmentNicholasNo ratings yet
- Neutropenic SepsisDocument38 pagesNeutropenic SepsisYS NateNo ratings yet
- Cytochemical StainsDocument4 pagesCytochemical StainsMartin PinedaNo ratings yet
- Microbiology Exam 3Document9 pagesMicrobiology Exam 3Sam SchlueterNo ratings yet
- Jurnal SepsisDocument13 pagesJurnal SepsisDwx PrasetyaNo ratings yet
- Dark FieldDocument41 pagesDark FieldAndré Amorim100% (2)
- Fisiopatología de La Meningitis BacterianaDocument7 pagesFisiopatología de La Meningitis BacterianaGiuliano AlbizziNo ratings yet
- Heamatology 1Document57 pagesHeamatology 1Victoria &BeautifulPeopleNo ratings yet
- Fundamentals of Nursing TestDocument78 pagesFundamentals of Nursing TestNicomille T. Caliging80% (5)