You might also like
- Coronavirus Disinfection in HistopathologyDocument4 pagesCoronavirus Disinfection in Histopathologywenyinrianto100% (1)
- Bprs Management of Children Admitted To Hospital With Covid19 - 20200319Document15 pagesBprs Management of Children Admitted To Hospital With Covid19 - 20200319Carla CANo ratings yet
- Radiol 2020201187 PDFDocument5 pagesRadiol 2020201187 PDFfikriafisNo ratings yet
- Paed COVID 19 Case P PUL 2020Document6 pagesPaed COVID 19 Case P PUL 2020Minaz PatelNo ratings yet
- Diagnostic Utility of Clinical Laboratory Data Determinations For Patients With The Severe COVID-19Document18 pagesDiagnostic Utility of Clinical Laboratory Data Determinations For Patients With The Severe COVID-19Carla CANo ratings yet
- Outpatient Management of Chronic Asthma in 2020: Clinical UpdateDocument2 pagesOutpatient Management of Chronic Asthma in 2020: Clinical UpdateCarla CANo ratings yet
- MainDocument37 pagesMainCarla CANo ratings yet
- Jain 2015Document12 pagesJain 2015Carla CANo ratings yet
- Boutin 2016 TransfusionDocument10 pagesBoutin 2016 TransfusionCarla CANo ratings yet
- 2006 ROME III. The Functional Gastrointestinal Disorders. GASTROENTEROLOGYDocument196 pages2006 ROME III. The Functional Gastrointestinal Disorders. GASTROENTEROLOGYCarla CANo ratings yet
- Autoimmune Hepatitis. JPGN 2009Document7 pagesAutoimmune Hepatitis. JPGN 2009Carla CANo ratings yet
- Finnie 2014 PatologiaDocument9 pagesFinnie 2014 PatologiaCarla CANo ratings yet
- Anaphylaxis in Children Cur Opin Pediatric 2016Document4 pagesAnaphylaxis in Children Cur Opin Pediatric 2016Carla CANo ratings yet
- Respiratory Disorders SDRRNDocument12 pagesRespiratory Disorders SDRRNCarla CANo ratings yet
- Neo Surfactante NejmDocument3 pagesNeo Surfactante NejmCarla CANo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- UMC Florida Annual Conference Filed ComplaintDocument36 pagesUMC Florida Annual Conference Filed ComplaintCasey Feindt100% (1)
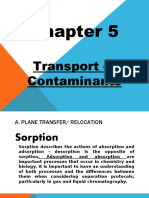
- Chapter 5Document11 pagesChapter 5XDXDXDNo ratings yet
- Aluminium FOil SearchDocument8 pagesAluminium FOil SearchAtul KumarNo ratings yet
- Weakness and Hypotonia: Prepared by DR Hodan Jama MDDocument38 pagesWeakness and Hypotonia: Prepared by DR Hodan Jama MDabdisalaan hassanNo ratings yet
- Chapter - 2 Fish MongeryDocument10 pagesChapter - 2 Fish MongeryKrishna ChaudharyNo ratings yet
- C ProgrammingDocument205 pagesC ProgrammingSrinivasan RamachandranNo ratings yet
- Teaching and Learning ResourcesDocument4 pagesTeaching and Learning ResourcesTey Lee PohNo ratings yet
- BSHM 23 ReviewerDocument8 pagesBSHM 23 ReviewerTrixie Mae MuncadaNo ratings yet
- Wicks Angela, Roethlein Christopher - A Satisfaction - Based Definition of QualityDocument1 pageWicks Angela, Roethlein Christopher - A Satisfaction - Based Definition of Qualityalfdjole0% (1)
- Essentials of Report Writing - Application in BusinessDocument28 pagesEssentials of Report Writing - Application in BusinessMahmudur Rahman75% (4)
- Nigerian Romance ScamDocument10 pagesNigerian Romance ScamAnonymous Pb39klJNo ratings yet
- Megneto TherapyDocument15 pagesMegneto TherapyedcanalNo ratings yet
- Isaac Asimov - "Nightfall"Document20 pagesIsaac Asimov - "Nightfall"Aditya Sharma100% (1)
- Reg OPSDocument26 pagesReg OPSAlexandru RusuNo ratings yet
- Going to the cinema listening practiceDocument2 pagesGoing to the cinema listening practiceMichael DÍligo Libre100% (1)
- Pathophysiology of Uremic EncephalopathyDocument5 pagesPathophysiology of Uremic EncephalopathyKristen Leigh Mariano100% (1)
- I. Specifikacija Opreme Sa Ugradnjom R.Br. Opis JM KomDocument4 pagesI. Specifikacija Opreme Sa Ugradnjom R.Br. Opis JM KomAleksandar VidakovicNo ratings yet
- A-00 IndexDocument10 pagesA-00 IndexNizarHamrouniNo ratings yet
- Subtracting-Fractions-Unlike DenominatorsDocument2 pagesSubtracting-Fractions-Unlike Denominatorsapi-3953531900% (1)
- UNIT- 5 IRSDocument78 pagesUNIT- 5 IRSganeshjaggineni1927No ratings yet
- Motor Operated ValveDocument6 pagesMotor Operated ValveYosses Sang NahkodaNo ratings yet
- Facebook TemplateDocument2 pagesFacebook Templateapi-352106462No ratings yet
- What Is Gross Income - Definition, Formula, Calculation, and ExampleDocument7 pagesWhat Is Gross Income - Definition, Formula, Calculation, and ExampleKapil SharmaNo ratings yet
- The Unseelie Prince Maze of Shadows Book 1 by Kathryn AnnDocument267 pagesThe Unseelie Prince Maze of Shadows Book 1 by Kathryn Annanissa Hri50% (2)
- Polygon shapes solve complex mechanical problemsDocument6 pagesPolygon shapes solve complex mechanical problemskristoffer_mosshedenNo ratings yet
- An IDEAL FLOW Has A Non-Zero Tangential Velocity at A Solid SurfaceDocument46 pagesAn IDEAL FLOW Has A Non-Zero Tangential Velocity at A Solid SurfaceJayant SisodiaNo ratings yet
- Supply Chain Management of VodafoneDocument8 pagesSupply Chain Management of VodafoneAnamika MisraNo ratings yet
- Chiller Carrier - 30gn-9siDocument28 pagesChiller Carrier - 30gn-9siZJ Limited (ZJLimited)No ratings yet
- Oxyacetylene Welding (OAW)Document26 pagesOxyacetylene Welding (OAW)athyrahNo ratings yet
- PronPack 5 Sample MaterialDocument13 pagesPronPack 5 Sample MaterialAlice FewingsNo ratings yet