You might also like
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Bias & ConfoundingDocument34 pagesBias & ConfoundingdrvikrantkabirpanthiNo ratings yet
- Chapter 9 Validity in Epidemiologic Studies Booklet - Final 9may2021Document7 pagesChapter 9 Validity in Epidemiologic Studies Booklet - Final 9may2021Genevieve Magpayo NangitNo ratings yet
- 4-Delgado Bias 2004Document8 pages4-Delgado Bias 2004Jairo Camilo Guevara FaríasNo ratings yet
- Bias, Confounding and Effect Modification in EpidemiologyDocument10 pagesBias, Confounding and Effect Modification in EpidemiologyCSilva16No ratings yet
- Bias in Research2Document16 pagesBias in Research2PashaNo ratings yet
- Epi & Biostats Review GuideDocument5 pagesEpi & Biostats Review GuideSamaneh Bolourchi100% (3)
- Epi BiasDocument4 pagesEpi BiascharlesNo ratings yet
- Delgado-Rodriguez 2004 SesgosDocument7 pagesDelgado-Rodriguez 2004 SesgosGaby SchwindtNo ratings yet
- Appraising The Evidence: What Is Selection Bias?: Case Control StudiesDocument2 pagesAppraising The Evidence: What Is Selection Bias?: Case Control Studiesruba azfr-aliNo ratings yet
- Validity of Epidemiological StudiesDocument11 pagesValidity of Epidemiological StudiesShruthi BhaskarNo ratings yet
- First AID For The USMLE Public HealthDocument20 pagesFirst AID For The USMLE Public HealthLilit M-yanNo ratings yet
- ANALYSIS OF CAUSE-EFFECT RELATIONSHIPSDocument50 pagesANALYSIS OF CAUSE-EFFECT RELATIONSHIPSRida AwwalNo ratings yet
- Nested Case Control StudyDocument6 pagesNested Case Control StudyFarah FarahNo ratings yet
- Biostatistics For CK Step 2 6.16.2019Document37 pagesBiostatistics For CK Step 2 6.16.2019karan kauraNo ratings yet
- Assessing Bias in Case-Control Studies: Comments, Opinions, and ReviewsDocument5 pagesAssessing Bias in Case-Control Studies: Comments, Opinions, and ReviewsAmelia MarisaNo ratings yet
- FA 2022 Small Size ExportDocument2 pagesFA 2022 Small Size Exportteyexes931No ratings yet
- Evaluating Sources of Bias in Epidemiologic StudiesDocument27 pagesEvaluating Sources of Bias in Epidemiologic StudiesAriyati MandiriNo ratings yet
- FA - Public Health ScienceDocument24 pagesFA - Public Health ScienceMargaret GraceNo ratings yet
- Nciph ERIC13Document3 pagesNciph ERIC13bejarhasanNo ratings yet
- 1408 BiasDocument3 pages1408 Biaspeppino WuverNo ratings yet
- Sepsis Mayor 35 AppDocument10 pagesSepsis Mayor 35 AppNatalia CruzNo ratings yet
- 3.1 Randomized Control Trials PDFDocument4 pages3.1 Randomized Control Trials PDFPia BustosNo ratings yet
- Bioe 211 - Causal InferenceDocument1 pageBioe 211 - Causal Inferencebabalegaspi09No ratings yet
- Primer Paper Cambio Alte Por Brue AppDocument32 pagesPrimer Paper Cambio Alte Por Brue AppAndres ChasiNo ratings yet
- Checklist Skin Assessment For NeonatesDocument12 pagesChecklist Skin Assessment For Neonatesapi-268617567No ratings yet
- Brief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk InfantsDocument34 pagesBrief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk InfantsCarlos CuadrosNo ratings yet
- IDC 213 06 Workshop 3 Critical Appraisal On Studies About HarmDocument5 pagesIDC 213 06 Workshop 3 Critical Appraisal On Studies About HarmFort SalvadorNo ratings yet
- Assessing Bias The Importance of Considering ConfoundingDocument4 pagesAssessing Bias The Importance of Considering ConfoundingAndrieli TodescatoNo ratings yet
- Cap. 7Document4 pagesCap. 7Familia CieletNo ratings yet
- BiasDocument62 pagesBiasLusungu S. LupenzaNo ratings yet
- CHAPTER 5 (Clinical Psych)Document7 pagesCHAPTER 5 (Clinical Psych)Elijah DiazNo ratings yet
- INTERNATIONAL JournalDocument6 pagesINTERNATIONAL JournalFitriNo ratings yet
- ERROR Pada STUDI EPIDEMIOLOGI GIZI KLINIKDocument27 pagesERROR Pada STUDI EPIDEMIOLOGI GIZI KLINIKIgus UlfayazeNo ratings yet
- A Meta-Analytic Examination of Attrition in Virtual Reality Exposure TherapyDocument9 pagesA Meta-Analytic Examination of Attrition in Virtual Reality Exposure TherapyArteria PsicosocialNo ratings yet
- Weekly Assignment Subject: Scientific Inquiry and Research Methodology ID: 8590 Submitted By: LaibaDocument4 pagesWeekly Assignment Subject: Scientific Inquiry and Research Methodology ID: 8590 Submitted By: LaibaPari VashNo ratings yet
- Internal Validity: The Ability of A Study To Measure What It Set Out To Measure Selection Bias: AreDocument3 pagesInternal Validity: The Ability of A Study To Measure What It Set Out To Measure Selection Bias: AreCA MNo ratings yet
- Nciph ERIC10Document5 pagesNciph ERIC10bejarhasanNo ratings yet
- 5 FMCH Research BiasDocument3 pages5 FMCH Research BiasMia CadizNo ratings yet
- Public Health FADocument22 pagesPublic Health FAsaurabhdhakedgNo ratings yet
- Chittaranjan, A. 2017Document4 pagesChittaranjan, A. 2017Andrea HenaoNo ratings yet
- Research VariablesDocument108 pagesResearch VariablesBagus Pande100% (1)
- Errors in Epidemiological StudiesDocument30 pagesErrors in Epidemiological StudiesFYMNo ratings yet
- PIIS0002937822011115Document2 pagesPIIS0002937822011115Maria Fernanda Sigcho ValenciaNo ratings yet
- Biostatistics Epidemiology Definitions ChartDocument10 pagesBiostatistics Epidemiology Definitions ChartM PatelNo ratings yet
- Systematic Error (Bias) : Types of Bias Non-Response Bias Healthy Worker Effect Berkson BiasDocument4 pagesSystematic Error (Bias) : Types of Bias Non-Response Bias Healthy Worker Effect Berkson BiasMarion SanchezNo ratings yet
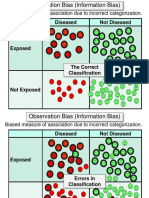
- Diseased Not Diseased: Biased Measure of Association Due To Incorrect CategorizationDocument11 pagesDiseased Not Diseased: Biased Measure of Association Due To Incorrect CategorizationJesus RodriguezNo ratings yet
- Sainani Et Al 2011 PM&RDocument5 pagesSainani Et Al 2011 PM&RHarshil DaveNo ratings yet
- 4 Bias and Causal Associations in Observational Research Grimes2002 PDFDocument5 pages4 Bias and Causal Associations in Observational Research Grimes2002 PDFBenor Amri MustaqimNo ratings yet
- Ebm Harm-EtiologyDocument49 pagesEbm Harm-EtiologyPapi BearNo ratings yet
- Epidemiology LectureDocument3 pagesEpidemiology Lecturekep1313No ratings yet
- 2017 - Cabilan & KynochDocument32 pages2017 - Cabilan & KynochazeemathmariyamNo ratings yet
- Chapter EightDocument66 pagesChapter EightYusuf JaferNo ratings yet
- Causal Decomposition of Hypertension Control DisparitiesDocument19 pagesCausal Decomposition of Hypertension Control DisparitieseswaynedNo ratings yet
- Bias in ResearchDocument45 pagesBias in ResearchIheakachi IheakachiNo ratings yet
- A Comparison of The Performance of ChildDocument8 pagesA Comparison of The Performance of Childiyanali7177No ratings yet
- Bias in Research: DR Aamer NaeemDocument16 pagesBias in Research: DR Aamer NaeembkdfiesefllNo ratings yet
- Critical Apprasial EbmDocument64 pagesCritical Apprasial Ebmsharma tobingNo ratings yet
- Threats To Research Bias and Error Confounding and InteractionDocument8 pagesThreats To Research Bias and Error Confounding and Interactionnajdah_220754970No ratings yet
- BiasDocument17 pagesBiasRanda IlhamNo ratings yet
- E249 FullDocument6 pagesE249 FullbejarhasanNo ratings yet
- Demand and Willingnesstopay For Health Insurance - Wageningen University and Research 272347Document106 pagesDemand and Willingnesstopay For Health Insurance - Wageningen University and Research 272347bejarhasanNo ratings yet
- AfrJMedHealthSci15118-8265798 225737Document6 pagesAfrJMedHealthSci15118-8265798 225737bejarhasanNo ratings yet
- Extension of Mandatory Health Insurance To Informal Sector Workers in TogoDocument14 pagesExtension of Mandatory Health Insurance To Informal Sector Workers in TogobejarhasanNo ratings yet
- Calculating Willingness-To-Pay As A Function of Biophysical WaterDocument74 pagesCalculating Willingness-To-Pay As A Function of Biophysical WaterbejarhasanNo ratings yet
- Adolescents' Knowledge of Their Health Insurance Coverage: Original ArticleDocument7 pagesAdolescents' Knowledge of Their Health Insurance Coverage: Original ArticlebejarhasanNo ratings yet
- An Estimation of The Willingness To Pay For Community Healthcare Insurance Scheme in Rural NigeriaDocument50 pagesAn Estimation of The Willingness To Pay For Community Healthcare Insurance Scheme in Rural NigeriabejarhasanNo ratings yet
- DownloadDocument46 pagesDownloadbejarhasanNo ratings yet
- 1 1Document7 pages1 1PARTH PATELNo ratings yet
- Ipi 161506Document11 pagesIpi 161506M Faozi KurniawanNo ratings yet
- Appleby Colostate 0053N 11190Document97 pagesAppleby Colostate 0053N 11190bejarhasanNo ratings yet
- Willingness to Pay for National Health Insurance in Saudi ArabiaDocument13 pagesWillingness to Pay for National Health Insurance in Saudi ArabiabejarhasanNo ratings yet
- Willingness To Pay For Rural Health Insurance: Evidence From Three African CountriesDocument309 pagesWillingness To Pay For Rural Health Insurance: Evidence From Three African CountriesbejarhasanNo ratings yet
- Adolescents' Knowledge of Their Health Insurance Coverage: Original ArticleDocument7 pagesAdolescents' Knowledge of Their Health Insurance Coverage: Original ArticlebejarhasanNo ratings yet
- Adolescents' Knowledge of Their Health Insurance Coverage: Original ArticleDocument7 pagesAdolescents' Knowledge of Their Health Insurance Coverage: Original ArticlebejarhasanNo ratings yet
- AfrJMedHealthSci15118-8265798 225737Document6 pagesAfrJMedHealthSci15118-8265798 225737bejarhasanNo ratings yet
- Adolescents' Knowledge of Their Health Insurance Coverage: Original ArticleDocument7 pagesAdolescents' Knowledge of Their Health Insurance Coverage: Original ArticlebejarhasanNo ratings yet
- Willingness to Pay for National Health Insurance in Saudi ArabiaDocument13 pagesWillingness to Pay for National Health Insurance in Saudi ArabiabejarhasanNo ratings yet
- This Content Downloaded From 185.136.149.13 On Sun, 27 Dec 2020 22:38:25 UTCDocument13 pagesThis Content Downloaded From 185.136.149.13 On Sun, 27 Dec 2020 22:38:25 UTCbejarhasanNo ratings yet
- Extension of Mandatory Health Insurance To Informal Sector Workers in TogoDocument14 pagesExtension of Mandatory Health Insurance To Informal Sector Workers in TogobejarhasanNo ratings yet
- REVISED00 Mal 0 Employment 0 FINALDocument86 pagesREVISED00 Mal 0 Employment 0 FINALbejarhasanNo ratings yet
- Research ArticleDocument9 pagesResearch ArticlebejarhasanNo ratings yet
- en Willingness To Pay and Ability To Pay FoDocument5 pagesen Willingness To Pay and Ability To Pay FobejarhasanNo ratings yet
- This Content Downloaded From 185.136.149.226 On Sat, 02 Jan 2021 20:03:20 UTCDocument8 pagesThis Content Downloaded From 185.136.149.226 On Sat, 02 Jan 2021 20:03:20 UTCbejarhasanNo ratings yet
- Willingness To Pay For Social Health Insurance Among Informal Sector Workers in Wuhan, China: A Contingent Valuation StudyDocument17 pagesWillingness To Pay For Social Health Insurance Among Informal Sector Workers in Wuhan, China: A Contingent Valuation StudybejarhasanNo ratings yet
- en Willingness To Pay and Ability To Pay FoDocument5 pagesen Willingness To Pay and Ability To Pay FobejarhasanNo ratings yet
- How Consumers' Willingness To Pay Is Measured in Practice: An Empirical Analysis of Common Approaches' RelevanceDocument8 pagesHow Consumers' Willingness To Pay Is Measured in Practice: An Empirical Analysis of Common Approaches' RelevancebejarhasanNo ratings yet
- Willingness Pay:: Valid and Reliable Measure of Health State Preference?Document9 pagesWillingness Pay:: Valid and Reliable Measure of Health State Preference?bejarhasanNo ratings yet
- Willingness To Pay For What? A Note On Alternative Definitions of Health Care Program Benefits For Contingent Valuation StudiesDocument5 pagesWillingness To Pay For What? A Note On Alternative Definitions of Health Care Program Benefits For Contingent Valuation StudiesbejarhasanNo ratings yet
- Nanna2011Document259 pagesNanna2011bejarhasanNo ratings yet
- Sick Sinus Syndrome ExplainedDocument12 pagesSick Sinus Syndrome ExplainedlauraNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsPrabhat KumarNo ratings yet
- The Crude and Adjusted Rates in Epidemiology PDFDocument9 pagesThe Crude and Adjusted Rates in Epidemiology PDFaliriorodrigoNo ratings yet
- Self Declaration Form Details For International Arriving PassengersDocument2 pagesSelf Declaration Form Details For International Arriving Passengersmahmudur rahmanNo ratings yet
- Virtual AOMC-PIN Meeting Focuses on Neuro AdvancesDocument34 pagesVirtual AOMC-PIN Meeting Focuses on Neuro AdvancesAomc Pin PerdossiNo ratings yet
- Complement Deficiencies NotesDocument5 pagesComplement Deficiencies NotesZeniaNo ratings yet
- COVID-19 - Informative EssayDocument1 pageCOVID-19 - Informative EssayRydl Pnp100% (1)
- CRP SensitivityDocument1 pageCRP SensitivityFadhilah CulanNo ratings yet
- Down Syndrome: Mugemana Henri Paterne Supervised by Prof DR Hoda GhareebDocument20 pagesDown Syndrome: Mugemana Henri Paterne Supervised by Prof DR Hoda GhareebPaterne MugemanaNo ratings yet
- COVID 19 Task Team DR Eba PashaDocument10 pagesCOVID 19 Task Team DR Eba PashaIsmail SlimNo ratings yet
- CombiflamDocument1 pageCombiflamRameshNo ratings yet
- Parkinson's DiseaseDocument19 pagesParkinson's DiseasedrtantryNo ratings yet
- Human Nocardia Infections: A Review of Pulmonary NocardiosisDocument7 pagesHuman Nocardia Infections: A Review of Pulmonary NocardiosisAyu Nurislami WulandariNo ratings yet
- Acute Management of Croup in The Emergency - Canadian Paediatric SocietyDocument6 pagesAcute Management of Croup in The Emergency - Canadian Paediatric SocietyHarrisNo ratings yet
- Jurnal SinusitisDocument49 pagesJurnal SinusitisAramanda Dian100% (1)
- Infection Prevention and Control at NICU Slide Deck 2.8.2018 PDFDocument134 pagesInfection Prevention and Control at NICU Slide Deck 2.8.2018 PDFRevathi DadamNo ratings yet
- Cardiorespiratory Conditioning in The Quality of LifeDocument4 pagesCardiorespiratory Conditioning in The Quality of LifeJani Cleria BezerraNo ratings yet
- PNLEDocument35 pagesPNLECharm TanyaNo ratings yet
- F8DB F089:Fungal InfectionsDocument6 pagesF8DB F089:Fungal InfectionsPharmacist Ehab HammadNo ratings yet
- Lecture 8 - SCI 8007SEF Medical Microbiology & Virology-Virology II - 2023Document76 pagesLecture 8 - SCI 8007SEF Medical Microbiology & Virology-Virology II - 2023YY CheungNo ratings yet
- Triangle of Human Ecology Theory Explains Environmental Spread of Infectious DiseasesDocument6 pagesTriangle of Human Ecology Theory Explains Environmental Spread of Infectious DiseasesClarissa Marie Limmang100% (1)
- Different Types of Diseases/disorders of The Nervous System.Document23 pagesDifferent Types of Diseases/disorders of The Nervous System.Saba Parvin Haque100% (4)
- P3 MicroDocument14 pagesP3 MicroDaniel GalitzineNo ratings yet
- IBS CaseDocument8 pagesIBS CaseStarr NewmanNo ratings yet
- Public Health Model PptDocument10 pagesPublic Health Model PptSurendra SanapNo ratings yet
- BP - Post Polio SyndromeDocument8 pagesBP - Post Polio Syndromeapi-26005027No ratings yet
- Hospital Linen ManagementDocument2 pagesHospital Linen Managementsrngm100% (1)
- SF 8 Learner Health ReportDocument2 pagesSF 8 Learner Health ReportKeian EstalaneNo ratings yet
- Levels of competent: 4 - Chronic gastritis causes and treatmentsDocument15 pagesLevels of competent: 4 - Chronic gastritis causes and treatmentsAndi Nurul Abidah RamliNo ratings yet
- Epa HQ Opp 2016 0385 0094 PDFDocument227 pagesEpa HQ Opp 2016 0385 0094 PDFuncleadolphNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityFrom EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityRating: 4.5 out of 5 stars4.5/5 (109)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)