You might also like
- Jurnal Kortikosteroid PDFDocument9 pagesJurnal Kortikosteroid PDFindry_purnamasari0% (1)
- Intranasal Corticosteroids in Management of Acute Sinusitis: A Systematic Review and Meta-AnalysisDocument9 pagesIntranasal Corticosteroids in Management of Acute Sinusitis: A Systematic Review and Meta-AnalysisagustinadianasariaguNo ratings yet
- Genetic Deteriminat of Asthma Acute Therapy in ChildrenDocument8 pagesGenetic Deteriminat of Asthma Acute Therapy in ChildrenTiar OktavianNo ratings yet
- Research: Corticosteroids For Pain Relief in Sore Throat: Systematic Review and Meta-AnalysisDocument7 pagesResearch: Corticosteroids For Pain Relief in Sore Throat: Systematic Review and Meta-AnalysiswindaintanpNo ratings yet
- Tos CronicaDocument12 pagesTos CronicasaloNo ratings yet
- Bukan jurnal-TreatmentMaxillarySinusitis2014FebDocument1 pageBukan jurnal-TreatmentMaxillarySinusitis2014FebagustinadianasariaguNo ratings yet
- J Clinic Periodontology - 2020 - Herrera - Adjunctive Effect of Locally Delivered Antimicrobials in Periodontitis TherapyDocument18 pagesJ Clinic Periodontology - 2020 - Herrera - Adjunctive Effect of Locally Delivered Antimicrobials in Periodontitis TherapyDr.Niveditha SNo ratings yet
- 1945892419851312Document10 pages1945892419851312kasandraharahapNo ratings yet
- Risk Factors For Drug-Resistant Streptococcus Pneumoniae and Antibiotic Prescribing Practices in Outpatient Community-Acquired PneumoniaDocument4 pagesRisk Factors For Drug-Resistant Streptococcus Pneumoniae and Antibiotic Prescribing Practices in Outpatient Community-Acquired PneumoniakingkinresmytaNo ratings yet
- Methods: Thomas Seagraves, MD Michael Gottlieb, MD Data SourcesDocument3 pagesMethods: Thomas Seagraves, MD Michael Gottlieb, MD Data SourcesJorge BarriosNo ratings yet
- Contro Pacientes DiabeticosDocument3 pagesContro Pacientes DiabeticosFrancisco Josue TinajeroNo ratings yet
- Pneumonia 4Document10 pagesPneumonia 4furqan92No ratings yet
- Probioticos Rinitis AlergicaDocument8 pagesProbioticos Rinitis AlergicaFlavio GuillenNo ratings yet
- J 1468-1331 2010 03092 XDocument10 pagesJ 1468-1331 2010 03092 XLauri VergaraNo ratings yet
- Translating Best Evidence Into Best CareDocument4 pagesTranslating Best Evidence Into Best CareJorge Vivanco RiosNo ratings yet
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- Impétigo Revisión SistemáticaDocument21 pagesImpétigo Revisión SistemáticaDanielNo ratings yet
- Sinusistis JAMA 2015Document14 pagesSinusistis JAMA 2015IvanCarrilloNo ratings yet
- Decadron vs. Pred in Ped AsthmaDocument7 pagesDecadron vs. Pred in Ped AsthmaAndrew JoshuaNo ratings yet
- PICU DDIsDocument8 pagesPICU DDIsFAHAD KHANNo ratings yet
- RCT Phenotypic Chronic RhinosinusitisDocument11 pagesRCT Phenotypic Chronic RhinosinusitisAyuNo ratings yet
- Contrato Riesgos Compartidos PDFDocument4 pagesContrato Riesgos Compartidos PDFSergio TerrasaNo ratings yet
- Inhaled Corticosteroids and The Occurrence of Oral CandidiasisDocument6 pagesInhaled Corticosteroids and The Occurrence of Oral CandidiasisSheila ParreirasNo ratings yet
- Nebulised Steroid in The Treatment of Croup: A Systematic Review of Randomised Controlled TrialsDocument7 pagesNebulised Steroid in The Treatment of Croup: A Systematic Review of Randomised Controlled TrialsSatriyo BagasNo ratings yet
- A Randomized Clinical TrialDocument11 pagesA Randomized Clinical TrialRandy PrayogoNo ratings yet
- Emerging Treatment Strategies For Impetigo in Endemic and Nonendemic Settings: A Systematic ReviewDocument21 pagesEmerging Treatment Strategies For Impetigo in Endemic and Nonendemic Settings: A Systematic Reviewnurul hidayatiNo ratings yet
- PDFDocument14 pagesPDFJardee DatsimaNo ratings yet
- 10.7326 m19-3007 GWCZDocument11 pages10.7326 m19-3007 GWCZmostafa shahrabiNo ratings yet
- Jurnal Pendukung 1.Document9 pagesJurnal Pendukung 1.Risky PerdanaNo ratings yet
- JRMS 18 43Document4 pagesJRMS 18 43Ricardo PietrobonNo ratings yet
- BMJ j3887 FullDocument10 pagesBMJ j3887 FullRiri Maisytoh PutriNo ratings yet
- Complementary Therapies in Medicine: Contents Lists Available atDocument13 pagesComplementary Therapies in Medicine: Contents Lists Available atAndi UmmahNo ratings yet
- Relative Efficacy of Systemic Treatments For Atopic DermatitisDocument10 pagesRelative Efficacy of Systemic Treatments For Atopic DermatitisRabia OmarNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- Influence of Psychological Stress On Non-Surgical Periodontal Treatment Outcomes in Patients With Severe Chronic PeriodontitisDocument10 pagesInfluence of Psychological Stress On Non-Surgical Periodontal Treatment Outcomes in Patients With Severe Chronic PeriodontitisAndra AgheorghieseiNo ratings yet
- Medical Therapy Versus Balloon Sinus Dilation in Adults With Chronic Rhinosinusitis (MERLOT) : 12-Month Follow-UpDocument9 pagesMedical Therapy Versus Balloon Sinus Dilation in Adults With Chronic Rhinosinusitis (MERLOT) : 12-Month Follow-UpNevyNo ratings yet
- Artic GotaDocument13 pagesArtic GotaAbraham MedinaNo ratings yet
- Efficacy of Extract of Pelargonium Sidoides in Children With Acute Non-Group A Beta-Hemolytic Streptococcus Tonsillopharyngitis: A Randomized, Double-Blind, Placebo-Controlled TrialDocument11 pagesEfficacy of Extract of Pelargonium Sidoides in Children With Acute Non-Group A Beta-Hemolytic Streptococcus Tonsillopharyngitis: A Randomized, Double-Blind, Placebo-Controlled TrialInnoVision Health Media100% (1)
- Effectiveness of Nebulized N-Acetylcysteine Solution in Children With Acute BronchiolitisDocument4 pagesEffectiveness of Nebulized N-Acetylcysteine Solution in Children With Acute BronchiolitisFiaz medicoNo ratings yet
- Do NotDocument8 pagesDo NotAkhmad AfriantoNo ratings yet
- Amoxicillin For Acute RhinosinusitisDocument16 pagesAmoxicillin For Acute RhinosinusitisShafa Khayla AzzahraNo ratings yet
- Herrera 2012 at BDocument11 pagesHerrera 2012 at BOfara PachecoNo ratings yet
- Jurnal RhinosinusitisDocument26 pagesJurnal RhinosinusitisFarah F SifakNo ratings yet
- TB 2Document11 pagesTB 2giant nitaNo ratings yet
- Paper Alumnos 3 PDFDocument10 pagesPaper Alumnos 3 PDFVictor Martinez HagenNo ratings yet
- Huang 2019Document11 pagesHuang 2019gekwahyuNo ratings yet
- Ordi-Ros J, Et Al, 2017.Document8 pagesOrdi-Ros J, Et Al, 2017.Suhenri SiahaanNo ratings yet
- Int Forum Allergy Rhinol - 2017 - Levy - Defining The Minimal Clinically Important Difference For Olfactory Outcomes in TheDocument6 pagesInt Forum Allergy Rhinol - 2017 - Levy - Defining The Minimal Clinically Important Difference For Olfactory Outcomes in TheSid TNo ratings yet
- FULLTEXT01Document21 pagesFULLTEXT01mason.sadeghiNo ratings yet
- CAP Treatamnet AcortadoDocument8 pagesCAP Treatamnet Acortadoapi-3707490No ratings yet
- 16 RaDocument10 pages16 RaNitish TankNo ratings yet
- E187 FullDocument7 pagesE187 FullVisaraNo ratings yet
- P0581 548 Risk Factors of Severity of Dengue.639Document1 pageP0581 548 Risk Factors of Severity of Dengue.639Hendri HariyantoNo ratings yet
- LeprosyDocument20 pagesLeprosyHafiz Sulistio UtomoNo ratings yet
- Javier Garrido - Esteroides en Enf Resp PDFDocument7 pagesJavier Garrido - Esteroides en Enf Resp PDFangelicapynNo ratings yet
- Medical Treatment of EpilepsyDocument17 pagesMedical Treatment of EpilepsyArbey Aponte PuertoNo ratings yet
- Complementary Therapies in Medicine: ReviewDocument7 pagesComplementary Therapies in Medicine: ReviewHielmy Auliya HasyimNo ratings yet
- Atopic Dermatitis ArticleDocument10 pagesAtopic Dermatitis ArticleKKNo ratings yet
- Clinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareFrom EverandClinical Updates in the Management of Severe Asthma: New Strategies for Individualizing Long-term CareNo ratings yet
- Decision Analytics and Optimization in Disease Prevention and TreatmentFrom EverandDecision Analytics and Optimization in Disease Prevention and TreatmentNan KongNo ratings yet
- VaazDocument1 pageVaazBudi KhangNo ratings yet
- Chapter 11: Hypertension, Chronic Kidney Disease, and The ElderlyDocument5 pagesChapter 11: Hypertension, Chronic Kidney Disease, and The ElderlyBudi KhangNo ratings yet
- PAMW 2013-7-8 TomasikDocument8 pagesPAMW 2013-7-8 TomasikBudi KhangNo ratings yet
- Hepatobilliary Ascariasis: Budi 406152021 Pembimbing: Dr. Lisa Irawati, Sp. RadDocument25 pagesHepatobilliary Ascariasis: Budi 406152021 Pembimbing: Dr. Lisa Irawati, Sp. RadBudi KhangNo ratings yet
- Seventh Report of The Joint National Committee On Prevention PDFDocument47 pagesSeventh Report of The Joint National Committee On Prevention PDFfitrah fajrianiNo ratings yet
- WEF The Economics of Non Disease Indonesia 2015 PDFDocument16 pagesWEF The Economics of Non Disease Indonesia 2015 PDFBudi KhangNo ratings yet
- Prevention of Blindness in Leprosy: An Overview of The Relevant Clinical and Programme-Planning IssuesDocument9 pagesPrevention of Blindness in Leprosy: An Overview of The Relevant Clinical and Programme-Planning IssuesBudi KhangNo ratings yet
- Case Report: Repetitive Breech Presentations at TermDocument5 pagesCase Report: Repetitive Breech Presentations at TermBudi KhangNo ratings yet
- Ref 4Document90 pagesRef 4Budi KhangNo ratings yet
- Physiologic Changes During Pregnancy and DeliveryDocument13 pagesPhysiologic Changes During Pregnancy and DeliveryBudi Khang100% (1)
- Journal Reading Risk Factor of PretermDocument23 pagesJournal Reading Risk Factor of PretermBudi KhangNo ratings yet
- General Practice: Risk of Otitis After AeruginosaDocument4 pagesGeneral Practice: Risk of Otitis After AeruginosaBudi KhangNo ratings yet
- Which Antibiotics Lead To Higher Clinical Cure Rates in Adults With Acute Maxillary Sinusitis?Document1 pageWhich Antibiotics Lead To Higher Clinical Cure Rates in Adults With Acute Maxillary Sinusitis?Budi KhangNo ratings yet
- 6 PubertasDocument70 pages6 PubertasBudi KhangNo ratings yet
- PNF 8th EditionDocument7 pagesPNF 8th EditionDanisaWajeNo ratings yet
- Opioid Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineDocument16 pagesOpioid Poisoning: by Dr. Daud Jabbar Taib Department of Forensic MedicineM KNo ratings yet
- Migraine FlowchartDocument2 pagesMigraine FlowchartKemunto OnchwariNo ratings yet
- Anxiolytics: Mr. Harshad Khade Msc. Medical Technology (Ota) Symbiosis International University, PuneDocument11 pagesAnxiolytics: Mr. Harshad Khade Msc. Medical Technology (Ota) Symbiosis International University, PuneHarshad KhadeNo ratings yet
- Prepared By: Manisha Thapa Leeza ShresthaDocument12 pagesPrepared By: Manisha Thapa Leeza ShresthaManjesh Mishra XettriNo ratings yet
- Rational Use of Drugs-IDocument38 pagesRational Use of Drugs-IUmair Mazhar100% (1)
- Clinical Review: Tablet Splitting: A Review of Weight and Content UniformityDocument12 pagesClinical Review: Tablet Splitting: A Review of Weight and Content Uniformitymukesh choudharyNo ratings yet
- Medical Chemistry 2 QUESTION BANKDocument9 pagesMedical Chemistry 2 QUESTION BANKAryan TripathiNo ratings yet
- Reading Sub-Test - Question Paper: Part ADocument4 pagesReading Sub-Test - Question Paper: Part AShyju Paul50% (4)
- PHA2020 - Nursing Pharmacology 1 Course Outline 2021Document4 pagesPHA2020 - Nursing Pharmacology 1 Course Outline 2021Alana CaballeroNo ratings yet
- Rhetoric Essay Super High MeDocument8 pagesRhetoric Essay Super High MeNeana LueckNo ratings yet
- Pharmacology (Intro-Drug Calculation)Document46 pagesPharmacology (Intro-Drug Calculation)May Chelle ErazoNo ratings yet
- Research Paper OutlineDocument3 pagesResearch Paper OutlineShateanu' Bryant100% (1)
- Paclitaxel Monograph-1 PDFDocument10 pagesPaclitaxel Monograph-1 PDFClaudia TiffanyNo ratings yet
- Opioid-Free AnesthesiaDocument8 pagesOpioid-Free AnesthesiaPaulina LugoNo ratings yet
- NSW Immunisation ScheduleDocument1 pageNSW Immunisation ScheduleKristinaNo ratings yet
- Drug Induced Skin DisordersDocument31 pagesDrug Induced Skin DisorderskeerthanaNo ratings yet
- Common Bacterial InfectionsDocument8 pagesCommon Bacterial Infectionsmits98No ratings yet
- PHARM 315: Cheza May Baldado BS Pharm IIIDocument12 pagesPHARM 315: Cheza May Baldado BS Pharm IIIKathleen B BaldadoNo ratings yet
- Supacfinal 110724233556 Phpapp01Document32 pagesSupacfinal 110724233556 Phpapp01varun rajNo ratings yet
- Prestem Suffixes 202003Document12 pagesPrestem Suffixes 202003Yachao LiuNo ratings yet
- Guidelines For ATC Classification and DDDDocument251 pagesGuidelines For ATC Classification and DDDJose De La Cruz De La ONo ratings yet
- Uti in WomenDocument8 pagesUti in WomenBhupesh KumarNo ratings yet
- Somna Clinical ReportDocument2 pagesSomna Clinical ReportcarebiphaNo ratings yet
- Lichen PlanusDocument6 pagesLichen PlanusMerry MiraNo ratings yet
- Medicine CanvassDocument4 pagesMedicine CanvassjomarNo ratings yet
- Garopride ManualDocument16 pagesGaropride Manualsherif_awadNo ratings yet
- Vietnam University of Traditional MedicineDocument9 pagesVietnam University of Traditional MedicineThu Huyền ĐinhNo ratings yet
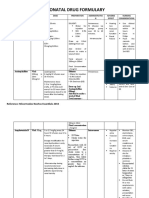
- Neonatal Drug FormularyDocument6 pagesNeonatal Drug FormularyLucian CaelumNo ratings yet
- Universal Medication Doctor Prescription Form TemplateDocument4 pagesUniversal Medication Doctor Prescription Form Templateshuiku xuiNo ratings yet