You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Exocad BookDocument16 pagesExocad BookHugoMoralesTecnicoDental50% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 6-C-RIIMPO301E - Conduct Hydraulic Excavator Operations - Learner Guide - V 1.1 02122019 PDFDocument31 pages6-C-RIIMPO301E - Conduct Hydraulic Excavator Operations - Learner Guide - V 1.1 02122019 PDFOwen PerrinNo ratings yet
- Bs en 00378 3 2016Document30 pagesBs en 00378 3 2016Darius VinNo ratings yet
- Straumann Screw Retained Hybrid RestorationsDocument36 pagesStraumann Screw Retained Hybrid RestorationsHugoMoralesTecnicoDentalNo ratings yet
- 100ah - 12V - 6FM100 VISIONDocument2 pages100ah - 12V - 6FM100 VISIONBashar SalahNo ratings yet
- Printing tips-MSLA-CastableCyanDocument3 pagesPrinting tips-MSLA-CastableCyanHugoMoralesTecnicoDentalNo ratings yet
- Scan Body REVIEW JPDDocument10 pagesScan Body REVIEW JPDHugoMoralesTecnicoDentalNo ratings yet
- SIMPLEX WhitePaper E Fin Low 2Document14 pagesSIMPLEX WhitePaper E Fin Low 2HugoMoralesTecnicoDentalNo ratings yet
- List of Orthodontic Functional AppliancesDocument6 pagesList of Orthodontic Functional AppliancesHugoMoralesTecnicoDentalNo ratings yet
- Implantsupportedoverdentures 160120191242Document121 pagesImplantsupportedoverdentures 160120191242HugoMoralesTecnicoDental100% (1)
- Manual Bego de Diseño y Colado de EstructurasDocument40 pagesManual Bego de Diseño y Colado de EstructurasHugoMoralesTecnicoDentalNo ratings yet
- Barras en ImplantologiaDocument5 pagesBarras en ImplantologiaHugoMoralesTecnicoDentalNo ratings yet
- Coachman Pink QDT 2010 PDFDocument15 pagesCoachman Pink QDT 2010 PDFHugoMoralesTecnicoDentalNo ratings yet
- Ceramics 2005Document26 pagesCeramics 2005Olariu FaneNo ratings yet
- RSGDocument5 pagesRSGHugoMoralesTecnicoDentalNo ratings yet
- Model-Based Guided Implant Surgery Planned PrecisionDocument6 pagesModel-Based Guided Implant Surgery Planned PrecisionHugoMoralesTecnicoDentalNo ratings yet
- Chapter 3Document31 pagesChapter 3HugoMoralesTecnicoDental100% (1)
- Attachments For Overdentures PDFDocument88 pagesAttachments For Overdentures PDFHugoMoralesTecnicoDental100% (1)
- Treatment Planning of The Edentulous Mandible PDFDocument9 pagesTreatment Planning of The Edentulous Mandible PDFHugoMoralesTecnicoDentalNo ratings yet
- Overdenture CompendiumDocument8 pagesOverdenture CompendiumHugoMoralesTecnicoDentalNo ratings yet
- Bar Locator Versus Bar Clip Attachment For Implant Assisted Mandibular Overdenture 2161 1122.S2 006Document5 pagesBar Locator Versus Bar Clip Attachment For Implant Assisted Mandibular Overdenture 2161 1122.S2 006HugoMoralesTecnicoDentalNo ratings yet
- BKLT DeaeratorDocument24 pagesBKLT Deaeratormalikgaurav01No ratings yet
- HiraDocument30 pagesHiravijay kumar singhNo ratings yet
- Structured ProgrammingDocument31 pagesStructured ProgrammingkakaboomNo ratings yet
- Gathering Network RequirementsDocument30 pagesGathering Network RequirementsAmin ZangetsuNo ratings yet
- Engine Maintenance PartsDocument13 pagesEngine Maintenance PartsSerkanAl100% (1)
- Kubernetes CommandsDocument36 pagesKubernetes CommandsOvigz Hero100% (2)
- Kinematics-03-Subjective SolvedDocument11 pagesKinematics-03-Subjective SolvedRaju SinghNo ratings yet
- Crankshaft Position (CKP) Sensor: 1F2-12 M161 Engine ControlsDocument6 pagesCrankshaft Position (CKP) Sensor: 1F2-12 M161 Engine ControlsKukuh SeptiantoNo ratings yet
- Doing Hot Work On Gas ShipDocument5 pagesDoing Hot Work On Gas ShipAnonymous icnhaNsFNo ratings yet
- Magneto Hydro Dynamics PresentationDocument19 pagesMagneto Hydro Dynamics PresentationVipul GuptaNo ratings yet
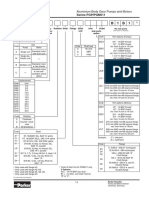
- PG 511 B 1 B 1: Ordering Code Series PGP/PGM511Document7 pagesPG 511 B 1 B 1: Ordering Code Series PGP/PGM511Four SticksNo ratings yet
- Fluid Mechanics Seventh Edition by Frank M. WhiteDocument1 pageFluid Mechanics Seventh Edition by Frank M. WhiteDarKaiserNo ratings yet
- BD+ CD+ XD+ - tcm833-3534072Document20 pagesBD+ CD+ XD+ - tcm833-3534072MisterMMNo ratings yet
- Curriculum Vitae: Augusto Javier Puican ZarpanDocument4 pagesCurriculum Vitae: Augusto Javier Puican Zarpanfrank_d_1No ratings yet
- Riscv SpecDocument32 pagesRiscv SpeckartimidNo ratings yet
- Gordon NovelDocument50 pagesGordon NovelNic Hotep100% (2)
- Estimate SR 14-15 02 KHANDEKARDocument5 pagesEstimate SR 14-15 02 KHANDEKARAkshay SavvasheriNo ratings yet
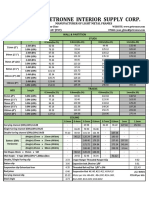
- Ultra Petronne Interior Supply Corp.: Manufacturer of Light Metal FramesDocument1 pageUltra Petronne Interior Supply Corp.: Manufacturer of Light Metal Framesjun vincint geleraNo ratings yet
- BM 81004 MuvDocument52 pagesBM 81004 MuvHamza Abbasi AbbasiNo ratings yet
- Good Practices in Government Resource Planning, Developed Vs Developing CountriesDocument11 pagesGood Practices in Government Resource Planning, Developed Vs Developing CountriesFreeBalanceGRPNo ratings yet
- PBLauncherDocument50 pagesPBLauncherborreveroNo ratings yet
- Mimaki Install Guide (En)Document16 pagesMimaki Install Guide (En)หน่อง นพดลNo ratings yet
- Write An Algorithm and Flowchart For Computing The Average Number of The Default 4 NumbersDocument3 pagesWrite An Algorithm and Flowchart For Computing The Average Number of The Default 4 NumbersMark Jelan100% (1)
- Transmisor HarrisDocument195 pagesTransmisor HarrisJose Juan Gutierrez Sanchez100% (1)
- Tube Well Design Project SolutionDocument5 pagesTube Well Design Project SolutionEng Ahmed abdilahi IsmailNo ratings yet
- Lesson Plan 2 Road FurnitureDocument4 pagesLesson Plan 2 Road FurnitureShahbaz SharifNo ratings yet