You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
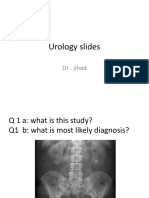
- Urology Slides: DR - JihadDocument4 pagesUrology Slides: DR - JihadJihad Anad100% (1)
- Urology Slides: DR - JihadDocument4 pagesUrology Slides: DR - JihadJihad Anad100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Vet PrepDocument9 pagesVet PrepAngel InzuastiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
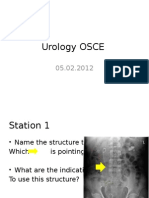
- Urology OSCEDocument9 pagesUrology OSCEJihad Anad75% (4)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ultrasound NotesDocument19 pagesUltrasound NotesJihad Anad100% (1)
- 500 Mcqs Surgery and RadiologyDocument66 pages500 Mcqs Surgery and RadiologyJihad Anad81% (59)
- Aleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Document14 pagesAleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Jihad AnadNo ratings yet
- Hydatidiform MoleDocument2 pagesHydatidiform MolePaola AgustinNo ratings yet
- ChoeDocument116 pagesChoeJihad AnadNo ratings yet
- ValiumDocument1 pageValiumKatie McPeekNo ratings yet
- Cleft Lip and Cleft PalateDocument22 pagesCleft Lip and Cleft PalateOm VaishNav0% (1)
- Van de Graaff GeneratorDocument10 pagesVan de Graaff GeneratorJihad AnadNo ratings yet
- MCQ RadiologyDocument10 pagesMCQ RadiologyJihad Anad100% (2)
- Kandungan Buku Perinatal Care Manual 4th Edition - 1jun2022Document14 pagesKandungan Buku Perinatal Care Manual 4th Edition - 1jun2022Zarif SyafiqNo ratings yet
- Reducing Waiting Time in OPD, Fortis Escort2Document12 pagesReducing Waiting Time in OPD, Fortis Escort2Janardhan Thokchom100% (2)
- Pre-Eclampsia and EclampsiaDocument21 pagesPre-Eclampsia and EclampsiaTamratKelelegn100% (1)
- HCP Chapterwise MCQ FinalDocument36 pagesHCP Chapterwise MCQ Finalsudeep kulkarni100% (7)
- Uro SepsisDocument23 pagesUro SepsisJihad Anad100% (1)
- Irrigating Fluids in Endoscopic Surgery: ReviewDocument12 pagesIrrigating Fluids in Endoscopic Surgery: ReviewJihad AnadNo ratings yet
- JSCFE Guidance Notes For Applicants - GenericDocument2 pagesJSCFE Guidance Notes For Applicants - GenericJihad AnadNo ratings yet
- Penile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceDocument4 pagesPenile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceJihad AnadNo ratings yet
- JSCFE Guidance Notes For Referees - GenericDocument2 pagesJSCFE Guidance Notes For Referees - GenericJihad AnadNo ratings yet
- Answer For Urology MCQDocument1 pageAnswer For Urology MCQJihad AnadNo ratings yet
- Antibiotics: by Dr. Jihad AnadDocument89 pagesAntibiotics: by Dr. Jihad AnadJihad AnadNo ratings yet
- DiureticsDocument6 pagesDiureticsJihad AnadNo ratings yet
- AbstractDocument2 pagesAbstractJihad AnadNo ratings yet
- ChoeDocument116 pagesChoeJihad AnadNo ratings yet
- Success With Penile Prosthesis From Patient'S ViewpointDocument3 pagesSuccess With Penile Prosthesis From Patient'S ViewpointJihad AnadNo ratings yet
- Appendix E: Microsoft Excel 2010 and Tools For Statistical AnalysisDocument15 pagesAppendix E: Microsoft Excel 2010 and Tools For Statistical AnalysisJihad AnadNo ratings yet
- AFP Vision 2028: A World-Class Armed Forces, Source of National PrideDocument2 pagesAFP Vision 2028: A World-Class Armed Forces, Source of National PrideLevy Garcia SanchezNo ratings yet
- Hioerplasia Mamaria GestacionalDocument9 pagesHioerplasia Mamaria GestacionalOctavio LeyvaNo ratings yet
- Ear Irrigation GuidelinesDocument11 pagesEar Irrigation Guidelinespramod454992No ratings yet
- Enema Administration: Size of Rectal TubeDocument3 pagesEnema Administration: Size of Rectal TubeMabesNo ratings yet
- Asphyxia NeonatorumDocument35 pagesAsphyxia NeonatorumMuhammad RagilNo ratings yet
- Fund 1.19 Patient Positions - NRSNGDocument2 pagesFund 1.19 Patient Positions - NRSNGEzekiel IsolaNo ratings yet
- Ijphrd Journal July-Sep 2013 - 06-06-213 PDFDocument307 pagesIjphrd Journal July-Sep 2013 - 06-06-213 PDFp1843dNo ratings yet
- Treatment Strategies in PCOS Patients: OnlineDocument8 pagesTreatment Strategies in PCOS Patients: Onlinenurul hidayahNo ratings yet
- Soal Un UnsratDocument80 pagesSoal Un UnsratSuzetteNo ratings yet
- CLP SeminarDocument125 pagesCLP SeminarNiyati VerulkarNo ratings yet
- Color HandoutsDocument23 pagesColor HandoutsAndreea SlabuNo ratings yet
- Basal Body Temperature Monitoring Contraceptive MethodDocument5 pagesBasal Body Temperature Monitoring Contraceptive Methodpriya vermaNo ratings yet
- Arch BarDocument28 pagesArch BarFachrul Latif DentistNo ratings yet
- Web-Based Versus Home-Based Postnatal Psychoeducational Interventions For First-Time Mothers: A Randomised Controlled TrialDocument13 pagesWeb-Based Versus Home-Based Postnatal Psychoeducational Interventions For First-Time Mothers: A Randomised Controlled Trialnur fadhilahNo ratings yet
- Abigail Seidman TestimonyDocument7 pagesAbigail Seidman TestimonySpiritus_FilmsNo ratings yet
- Xylin Specialist ToothpasteDocument3 pagesXylin Specialist ToothpasteMarvin AngNo ratings yet
- Prefix, Suffix & Root ListDocument10 pagesPrefix, Suffix & Root Listfarrokh880No ratings yet
- Hospicio Hospital MargaoDocument27 pagesHospicio Hospital MargaoSanthoshNo ratings yet
- Pendekatan Diagnosis AnemiaDocument7 pagesPendekatan Diagnosis AnemiaFerry GhifariNo ratings yet
- Romania Fact SheetDocument2 pagesRomania Fact SheetEmeseDengNo ratings yet
- MagnitudeDocument91 pagesMagnitudesanthiyasandyNo ratings yet
- CV EnglishDocument2 pagesCV EnglishDAMIANNo ratings yet