You might also like
- Optimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsFrom EverandOptimizing Advanced Therapies in Ulcerative Colitis: Is Your Practice Up to Date? A Focus on Clinical Evidence and Guideline RecommendationsNo ratings yet
- EgebergDocument11 pagesEgebergluis moralesNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- MenterDocument11 pagesMenterluis moralesNo ratings yet
- Medication Adherence in Inflammatory Bowel Disease: ReviewDocument12 pagesMedication Adherence in Inflammatory Bowel Disease: ReviewVirgo WNo ratings yet
- Yeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisDocument9 pagesYeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisAndi MarsaliNo ratings yet
- Treatment Persistence of Ixekizumab in Adults With Moderate-to-Severe Plaque Psoriasis Participating in The Canadian Patient Support ProgramDocument10 pagesTreatment Persistence of Ixekizumab in Adults With Moderate-to-Severe Plaque Psoriasis Participating in The Canadian Patient Support ProgramRon VNo ratings yet
- Treatment of Pemphigus Vulgaris and Pemphigus FoliaceusDocument13 pagesTreatment of Pemphigus Vulgaris and Pemphigus FoliaceusMelly MayasariNo ratings yet
- Chao Chen Et Al - Real-World Pattern of Biologic Use in Patients With Inflammatory Bowel DiseaseDocument11 pagesChao Chen Et Al - Real-World Pattern of Biologic Use in Patients With Inflammatory Bowel DiseaseJLNo ratings yet
- Relative Efficacy of Systemic Treatments For Atopic DermatitisDocument10 pagesRelative Efficacy of Systemic Treatments For Atopic DermatitisRabia OmarNo ratings yet
- Double Blind Randomized Placebo-Controlled Trial To Evaluate The Efficacy and Safety of Short-Course Low Dose Oral Prednisolone in Pityriasis RoseaDocument10 pagesDouble Blind Randomized Placebo-Controlled Trial To Evaluate The Efficacy and Safety of Short-Course Low Dose Oral Prednisolone in Pityriasis RoseaSalsabila Munirah AmirNo ratings yet
- Yasmeen 2020Document16 pagesYasmeen 2020Rafaela Queiroz MascarenhasNo ratings yet
- 3.effects of Zingiber Officinalis (WILLD.)Document6 pages3.effects of Zingiber Officinalis (WILLD.)adil.shanuNo ratings yet
- 686 FullDocument9 pages686 FullEster DuwitNo ratings yet
- HepatologyDocument3 pagesHepatologywaldirNo ratings yet
- Long-Term Safety of Oral Systemic Therapies For Psoriasis: A Comprehensive Review of The LiteratureDocument25 pagesLong-Term Safety of Oral Systemic Therapies For Psoriasis: A Comprehensive Review of The Literaturefegita manopoNo ratings yet
- SCLUPTURE 5 Years Extension StudyDocument8 pagesSCLUPTURE 5 Years Extension StudyAndi MarsaliNo ratings yet
- Cancer Controversies Clinical Trials Confirm But Don't Innovate-ConDocument3 pagesCancer Controversies Clinical Trials Confirm But Don't Innovate-ConadssaNo ratings yet
- Complementary Therapies in Medicine: ReviewDocument7 pagesComplementary Therapies in Medicine: ReviewHielmy Auliya HasyimNo ratings yet
- Objectively Measured Vs Self-Reported Compliance During Oral Appliance Therapy For Sleep-Disordered BreathingDocument8 pagesObjectively Measured Vs Self-Reported Compliance During Oral Appliance Therapy For Sleep-Disordered Breathing陈延珑No ratings yet
- CAP 5 Day Treatment Duration Guidelines 091817Document8 pagesCAP 5 Day Treatment Duration Guidelines 091817Gita SupyanaNo ratings yet
- Chemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionDocument10 pagesChemotherapy-Associated Oral Sequelae in Patients With Cancers Outside The Head and Neck RegionNndaydnaNo ratings yet
- Norlin JM Et Al 2017. Real World Outcomes in 2646 Psoriasis Patients One in Five Has PASI 10 and or DLQI 10 Under Ongoing Systemic TherapyDocument6 pagesNorlin JM Et Al 2017. Real World Outcomes in 2646 Psoriasis Patients One in Five Has PASI 10 and or DLQI 10 Under Ongoing Systemic TherapyAndi MarsaliNo ratings yet
- Long-Term Survival in Childhood Acute Lymphocytic Leukemia in ItalyDocument4 pagesLong-Term Survival in Childhood Acute Lymphocytic Leukemia in ItalyhallowNo ratings yet
- HTTP WWW - Sciencedirect.com Science Ob MImg& Imagekey B6WP1-4HK01J7-7-1& Cdi 6977& User 8187385& OrigDocument4 pagesHTTP WWW - Sciencedirect.com Science Ob MImg& Imagekey B6WP1-4HK01J7-7-1& Cdi 6977& User 8187385& OrigBimalKrishnaNo ratings yet
- J Clinic Periodontology - 2020 - Herrera - Adjunctive Effect of Locally Delivered Antimicrobials in Periodontitis TherapyDocument18 pagesJ Clinic Periodontology - 2020 - Herrera - Adjunctive Effect of Locally Delivered Antimicrobials in Periodontitis TherapyDr.Niveditha SNo ratings yet
- Long-Term Safety Profile of Belimumab Plus Standard Therapy in Patients With Systemic Lupus ErythematosusDocument10 pagesLong-Term Safety Profile of Belimumab Plus Standard Therapy in Patients With Systemic Lupus Erythematosusperez juanNo ratings yet
- 13.effect of Omega-3 On Recurrent Aphthous Stomatitis and Improvement Quality of LifeDocument9 pages13.effect of Omega-3 On Recurrent Aphthous Stomatitis and Improvement Quality of LifeCoste Iulia RoxanaNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- teughels2020Document245 pagesteughels2020Josmell Campos MedinaNo ratings yet
- 6-Month MDT Therapy Effectiveness in PB LeprosyDocument27 pages6-Month MDT Therapy Effectiveness in PB LeprosyAlfonsusAlexNo ratings yet
- Efficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC StudyDocument1 pageEfficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC Studyjuloc34No ratings yet
- The Effect of Cryotherapy On The Prevention of Oral Mucositis and On TheDocument7 pagesThe Effect of Cryotherapy On The Prevention of Oral Mucositis and On ThePaola GilNo ratings yet
- 2012 Optical Tomography ML Flexman JBO 01Document9 pages2012 Optical Tomography ML Flexman JBO 01Data KiswaraNo ratings yet
- Adherence in Topical Treatment in PsoriasisDocument7 pagesAdherence in Topical Treatment in PsoriasisWei Sheng ChongNo ratings yet
- JOralMaxillofacPathol242344-2162961 060029Document8 pagesJOralMaxillofacPathol242344-2162961 060029PreethyNo ratings yet
- Rheumatology 05Document6 pagesRheumatology 05C Bala DiwakeshNo ratings yet
- j.eurpsy.2007.03.002Document11 pagesj.eurpsy.2007.03.002xhdrv7nvdrNo ratings yet
- Clinical Microbiology and InfectionDocument6 pagesClinical Microbiology and InfectionPutriNurulMuthiaNo ratings yet
- Chagas MetaanaliseDocument13 pagesChagas MetaanaliseDouglas CostaNo ratings yet
- Topical dapsone reduces flareups in folliculitis decalvansDocument2 pagesTopical dapsone reduces flareups in folliculitis decalvansRoxanne KapNo ratings yet
- The Effect of Long-Term Aspirin Intake On The Outcome of Non-Surgical Periodontal Therapy in Smokers: A Double-Blind, Randomized Pilot StudyDocument8 pagesThe Effect of Long-Term Aspirin Intake On The Outcome of Non-Surgical Periodontal Therapy in Smokers: A Double-Blind, Randomized Pilot StudyOctavian BoaruNo ratings yet
- Atorvastatin Improves Sputum Conversion and Chest X-Ray Severity ScoreDocument6 pagesAtorvastatin Improves Sputum Conversion and Chest X-Ray Severity Scorecharmainemargaret.parreno.medNo ratings yet
- Article 6Document8 pagesArticle 6Yasmine SlhNo ratings yet
- ITU Comparacion 7 - 14 Dias de TtoDocument9 pagesITU Comparacion 7 - 14 Dias de TtoJohana Zamudio RojasNo ratings yet
- Alifiani-Jurding SNNTDocument9 pagesAlifiani-Jurding SNNTYAHYA Al-HILALNo ratings yet
- Art 2Document21 pagesArt 2xdxdxdxdNo ratings yet
- Kees Tra 2014Document21 pagesKees Tra 2014Marco Antonio García LunaNo ratings yet
- Malfertheiner 2017 STW 5 Iberogast Therapy in Gastrointestinal Functional DisordersDocument5 pagesMalfertheiner 2017 STW 5 Iberogast Therapy in Gastrointestinal Functional DisordersbastomyNo ratings yet
- Immunotherapy in Non Small Cell Lung Cancer Facts and HopeDocument22 pagesImmunotherapy in Non Small Cell Lung Cancer Facts and HopeasdffdsaNo ratings yet
- Nebulised Steroid in The Treatment of Croup: A Systematic Review of Randomised Controlled TrialsDocument7 pagesNebulised Steroid in The Treatment of Croup: A Systematic Review of Randomised Controlled TrialsSatriyo BagasNo ratings yet
- Asthma Management by New Zealand Pharmac PDFDocument10 pagesAsthma Management by New Zealand Pharmac PDFReski Anugrahsari AsramNo ratings yet
- Endoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudyDocument6 pagesEndoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudySamuel0651No ratings yet
- PIIS0190962223031870Document10 pagesPIIS01909622230318705jnpzgz4cqNo ratings yet
- Management of Glucocorticoid-Induced OsteoporosisDocument19 pagesManagement of Glucocorticoid-Induced OsteoporosisNdhy Pharm HabibieNo ratings yet
- 16859604Document8 pages16859604Brent DoolanNo ratings yet
- BMJ j3887 FullDocument10 pagesBMJ j3887 FullRiri Maisytoh PutriNo ratings yet
- A Randomised Dose-Ranging Study of Tiotropium Respimat® in Children With Symptomatic Asthma Despite Inhaled CorticosteroidsDocument10 pagesA Randomised Dose-Ranging Study of Tiotropium Respimat® in Children With Symptomatic Asthma Despite Inhaled CorticosteroidsabdmaliknasNo ratings yet
- Amox + MetronidDocument2 pagesAmox + MetronidVlad LichiNo ratings yet
- Daftar Kelulusan Mcqs CBT Ukmppd Periode Agustus 2019Document113 pagesDaftar Kelulusan Mcqs CBT Ukmppd Periode Agustus 2019FarhanNo ratings yet
- Daftar Kelulusan Osce Periode Agustus 2017 PDFDocument115 pagesDaftar Kelulusan Osce Periode Agustus 2017 PDFRovanNo ratings yet
- I J P R S Ijprs: Nternational Ournal For Harmaceutical Esearch CholarsDocument5 pagesI J P R S Ijprs: Nternational Ournal For Harmaceutical Esearch CholarsChristman SihiteNo ratings yet
- 05 - 211acute Kidney Injury in Critically Ill Children at Pediatric Intensive Care UnitDocument4 pages05 - 211acute Kidney Injury in Critically Ill Children at Pediatric Intensive Care UnitChristman SihiteNo ratings yet
- Physical Therapy: Physical Therapy 2.0: Leveraging Social Media To Engage Patients in Rehabilitation and Health PromotionDocument24 pagesPhysical Therapy: Physical Therapy 2.0: Leveraging Social Media To Engage Patients in Rehabilitation and Health PromotionChristman SihiteNo ratings yet
- Trajectory MarvDocument9 pagesTrajectory MarvChristman SihiteNo ratings yet
- Psychiatric Rehabilitation ArticlesDocument8 pagesPsychiatric Rehabilitation ArticlesChristman SihiteNo ratings yet
- 4110Document72 pages4110Christman SihiteNo ratings yet
- Hydrogen Sulfide Protects From Colitis And.5Document12 pagesHydrogen Sulfide Protects From Colitis And.5Christman SihiteNo ratings yet
- Erratum: Ulcerative Colitis Practice Guidelines in Adults: American College of Gastroenterology, Practice Parameters CommitteeDocument24 pagesErratum: Ulcerative Colitis Practice Guidelines in Adults: American College of Gastroenterology, Practice Parameters CommitteeChristman SihiteNo ratings yet
- Immobilization: Dr. Rose Dinda Martini, SPPDDocument25 pagesImmobilization: Dr. Rose Dinda Martini, SPPDChristman SihiteNo ratings yet
- Chronic Otitis Media: Chunfu Dai M.D & Ph. D Otolaryngology Department Eye Ear Nose and Throat Hospital Fudan UniversityDocument25 pagesChronic Otitis Media: Chunfu Dai M.D & Ph. D Otolaryngology Department Eye Ear Nose and Throat Hospital Fudan UniversityChristman SihiteNo ratings yet
- Presentation 1Document1 pagePresentation 1Christman SihiteNo ratings yet
- Enlarged Peripheral Nerves On LeprosyDocument6 pagesEnlarged Peripheral Nerves On LeprosyGarrett SimpsonNo ratings yet
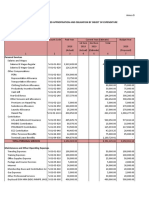
- Programmed Appropriation and Obligation by Object of ExpenditureDocument7 pagesProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoNo ratings yet
- MUHC News LetterDocument16 pagesMUHC News LetterLouiseWorrallNo ratings yet
- CH 13 MacFormDocument82 pagesCH 13 MacFormEdgar Campos LizárragaNo ratings yet
- Physical Fitness Components & Testing MethodsDocument6 pagesPhysical Fitness Components & Testing MethodsJopieNo ratings yet
- Rulerships and Qualities Anatomy and Physiology Correlated To The ZodiacDocument4 pagesRulerships and Qualities Anatomy and Physiology Correlated To The Zodiactushar100% (1)
- 07 The Molecular Biology of CancerDocument39 pages07 The Molecular Biology of CancerJustin GonzalesNo ratings yet
- 13 Suppl1Document31 pages13 Suppl1VinodNo ratings yet
- Appendix L HHRA CombinedDocument428 pagesAppendix L HHRA Combinedwholmes5924No ratings yet
- Loddon Mallee Regional Diabetes Pathways Version 2 PDFDocument30 pagesLoddon Mallee Regional Diabetes Pathways Version 2 PDFlatifa adluNo ratings yet
- Emergency MedicineDocument42 pagesEmergency Medicinedrliza75% (8)
- SmokingDocument29 pagesSmokingKris NNo ratings yet
- Zikes - Jaaha - 2012 - Bilateral Ventriculocordectomy Via Ventral Approach For LAR PARDocument11 pagesZikes - Jaaha - 2012 - Bilateral Ventriculocordectomy Via Ventral Approach For LAR PARranderson1972No ratings yet
- OesophagusDocument15 pagesOesophagusIBRAHEM JUMAHNo ratings yet
- S807 Mini Review v4Document37 pagesS807 Mini Review v4Daen de LeonNo ratings yet
- Breast MCQ Questions on Pathology Findings, Risk Factors and Treatment OptionsDocument55 pagesBreast MCQ Questions on Pathology Findings, Risk Factors and Treatment OptionsAhmad Adel Qaqour94% (16)
- Treatment of Pemphigus Vulgaris and Pemphigus FoliaceusDocument13 pagesTreatment of Pemphigus Vulgaris and Pemphigus FoliaceusMelly MayasariNo ratings yet
- Clinical guidelines for liver transplantationDocument53 pagesClinical guidelines for liver transplantationMadalina StoicescuNo ratings yet
- Can gray hair be donated for cancer wigsDocument1 pageCan gray hair be donated for cancer wigsDawa TsheringNo ratings yet
- Life Expectancy FactorsDocument3 pagesLife Expectancy FactorsRizza GonzagaNo ratings yet
- FBCA Biomarkers and ConditionsDocument8 pagesFBCA Biomarkers and Conditionsmet50% (2)
- STandPublicHealthinIndia Chap13 10282016 PDFDocument473 pagesSTandPublicHealthinIndia Chap13 10282016 PDFsdt4uxNo ratings yet
- Bio Medical Waste TheoryDocument14 pagesBio Medical Waste TheoryManish Kumawat100% (1)
- Callon - Hybrid ForumsDocument58 pagesCallon - Hybrid ForumsLuis HermosillaNo ratings yet
- Meat industry health and safety guidanceDocument205 pagesMeat industry health and safety guidanceJaime SilvaNo ratings yet
- PROGRAM - DETAILAT Conferinta Bioinginerie 2015 PDFDocument41 pagesPROGRAM - DETAILAT Conferinta Bioinginerie 2015 PDFAlina RogojanuNo ratings yet
- GP anger over Vit D testDocument2 pagesGP anger over Vit D testmonday125No ratings yet
- Icru 82Document67 pagesIcru 82Aditya DisdusNo ratings yet
- Annexure - A Incident Assessment Risk MatrixDocument4 pagesAnnexure - A Incident Assessment Risk MatrixDilshad aliNo ratings yet
- ChoeDocument116 pagesChoeJihad AnadNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)