You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Signnage 2022Document10 pagesSignnage 2022mariegold mortola fabelaNo ratings yet
- Macusi CDC-List-of-Enrolled-Children-2021-2022-for-Child-FriendlyDocument1 pageMacusi CDC-List-of-Enrolled-Children-2021-2022-for-Child-Friendlymariegold mortola fabelaNo ratings yet
- Centro Imelda CDC-List-of-Enrolled-Children-2021-2022-for-Child-FriendlyDocument2 pagesCentro Imelda CDC-List-of-Enrolled-Children-2021-2022-for-Child-Friendlymariegold mortola fabelaNo ratings yet
- Binacalan CDC-List-of-Enrolled-Children-2021-2022-for-Child-FriendlyDocument1 pageBinacalan CDC-List-of-Enrolled-Children-2021-2022-for-Child-Friendlymariegold mortola fabelaNo ratings yet
- Registration ListDocument1 pageRegistration Listmariegold mortola fabelaNo ratings yet
- IVLO CDC-List-of-Enrolled-Children-2021-2022-for-Child-FriendlyDocument4 pagesIVLO CDC-List-of-Enrolled-Children-2021-2022-for-Child-Friendlymariegold mortola fabelaNo ratings yet
- Dra - Marybelle Agravante - Linog: John Paolo Revira - CasiDocument1 pageDra - Marybelle Agravante - Linog: John Paolo Revira - Casimariegold mortola fabelaNo ratings yet
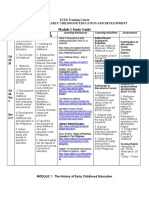
- ECED Module 1 - The History of Early Childhood EducationDocument7 pagesECED Module 1 - The History of Early Childhood Educationmariegold mortola fabelaNo ratings yet
- Narrative Report 2022Document1 pageNarrative Report 2022mariegold mortola fabelaNo ratings yet
- ECED Module 1 - Activity 1-4Document2 pagesECED Module 1 - Activity 1-4mariegold mortola fabelaNo ratings yet
- National Federation of Day Care Workers Position PapersDocument2 pagesNational Federation of Day Care Workers Position Papersmariegold mortola fabelaNo ratings yet
- Enrolment FormDocument1 pageEnrolment Formmariegold mortola fabelaNo ratings yet
- MONITORING REPORT 2022 AssessmentDocument5 pagesMONITORING REPORT 2022 Assessmentmariegold mortola fabelaNo ratings yet
- Pictures 1Document11 pagesPictures 1mariegold mortola fabelaNo ratings yet
- Form 2.1 (Temporary) Monthly Barangay Consolidated Monitoring Report On Outcome and Output IndicatorsDocument3 pagesForm 2.1 (Temporary) Monthly Barangay Consolidated Monitoring Report On Outcome and Output Indicatorsmariegold mortola fabelaNo ratings yet
- Omnibus Certification of Authenticity and Veracity of Documents 1Document1 pageOmnibus Certification of Authenticity and Veracity of Documents 1mariegold mortola fabelaNo ratings yet
- PDF PDS 2017Document4 pagesPDF PDS 2017mariegold mortola fabelaNo ratings yet
- Labels For Boxes 2Document10 pagesLabels For Boxes 2mariegold mortola fabelaNo ratings yet
- List of Enrolled Children 2021-2022 (For Child Friendly)Document2 pagesList of Enrolled Children 2021-2022 (For Child Friendly)mariegold mortola fabelaNo ratings yet
- Labels For BoxesDocument18 pagesLabels For Boxesmariegold mortola fabelaNo ratings yet
- Inventory ListDocument1 pageInventory Listmariegold mortola fabelaNo ratings yet
- Form 1.1 (Temporary) Monthly Outcome & Indicators - Center LevelDocument6 pagesForm 1.1 (Temporary) Monthly Outcome & Indicators - Center Levelmariegold mortola fabelaNo ratings yet
- Initial and Annual Health RecordDocument2 pagesInitial and Annual Health Recordmariegold mortola fabelaNo ratings yet
- List of Enrollees FormDocument2 pagesList of Enrollees Formmariegold mortola fabelaNo ratings yet
- Intake FormDocument3 pagesIntake Formmariegold mortola fabelaNo ratings yet
- DCW Action PlanDocument1 pageDCW Action Planmariegold mortola fabelaNo ratings yet
- Food Allocation MatrixDocument3 pagesFood Allocation Matrixmariegold mortola fabelaNo ratings yet
- Child Enrollment and Survey Form - PATAGDocument2 pagesChild Enrollment and Survey Form - PATAGmariegold mortola fabelaNo ratings yet
- Consent For Provision of Day Care ServiceDocument1 pageConsent For Provision of Day Care Servicemariegold mortola fabelaNo ratings yet
- Child Enrollment and Survey FormDocument2 pagesChild Enrollment and Survey Formmariegold mortola fabelaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 1.sarah W Chege Research Project August 2019Document72 pages1.sarah W Chege Research Project August 2019Getachew AddisuNo ratings yet
- Commercial Law AgencyDocument25 pagesCommercial Law AgencyAudreyAuYeungNo ratings yet
- Offer in Compromise: Form 656 BookletDocument28 pagesOffer in Compromise: Form 656 BookletAnonymous JRunUFTMbNo ratings yet
- Investment AvenuesDocument16 pagesInvestment AvenuesChitta PatiNo ratings yet
- MSC Essays - Active PurchasingDocument9 pagesMSC Essays - Active PurchasingAlbert DomingoNo ratings yet
- Cto 1Document4 pagesCto 1Rishu SrivastavaNo ratings yet
- Financial Planning & Wealth Management: Sunder Ram Korivi, National Institute of Securities Markets, Navi MumbaiDocument20 pagesFinancial Planning & Wealth Management: Sunder Ram Korivi, National Institute of Securities Markets, Navi MumbaijayaNo ratings yet
- Aviation Insurance: Aviation Insurance Is Insurance Coverage Geared Specifically To TheDocument10 pagesAviation Insurance: Aviation Insurance Is Insurance Coverage Geared Specifically To TheAbhishek TiwariNo ratings yet
- Business RiskDocument58 pagesBusiness RiskK GNo ratings yet
- Las# 5 - (Iaa) Error CorrectionDocument7 pagesLas# 5 - (Iaa) Error CorrectionStella MarieNo ratings yet
- October 16 EditionDocument36 pagesOctober 16 EditiontangramtechNo ratings yet
- By - Vansh Karel Class: 11 Com B ROLL:17Document17 pagesBy - Vansh Karel Class: 11 Com B ROLL:17VANSH KARELNo ratings yet
- CH 01Document28 pagesCH 01cushin2009No ratings yet
- World Bank Report-Road Transport Service EfficiencyDocument16 pagesWorld Bank Report-Road Transport Service EfficiencyPunit ChadhaNo ratings yet
- Radian Default Claims Servicing GuideDocument42 pagesRadian Default Claims Servicing GuidelostvikingNo ratings yet
- Insurance For Accidents Involving Third Parties or Their PropertyDocument4 pagesInsurance For Accidents Involving Third Parties or Their PropertyMaulana IbrahimNo ratings yet
- Annotated Bibliography Draft-1Document5 pagesAnnotated Bibliography Draft-1api-217663549No ratings yet
- CH-4 Subjective, Case Based, CBQ AssignmentDocument2 pagesCH-4 Subjective, Case Based, CBQ Assignmentֆաǟʍɛʋ ɢʊքƭǟNo ratings yet
- OCF-18 FillableDocument2 pagesOCF-18 FillableestakhrikarimNo ratings yet
- D096673877 7117287603297891 SchedulescDocument3 pagesD096673877 7117287603297891 SchedulescrakeshNo ratings yet
- Acord 125 (Updated) PDFDocument3 pagesAcord 125 (Updated) PDFAnonymous 14ZyLfZjuDNo ratings yet
- Premiums Earned of Non-Life Insurance CompaniesDocument2 pagesPremiums Earned of Non-Life Insurance CompaniesRon CatalanNo ratings yet
- A Project Report OnDocument54 pagesA Project Report Onnitinjadhav30No ratings yet
- VP Financial Planning Analysis in USA Resume John EffreinDocument2 pagesVP Financial Planning Analysis in USA Resume John EffreinJohnEffrein2No ratings yet
- VL Mock ExamDocument11 pagesVL Mock ExamJohnelle Ashley Baldoza TorresNo ratings yet
- Bid Document Volume II PKG 3 PDFDocument124 pagesBid Document Volume II PKG 3 PDFJ.S. RathoreNo ratings yet
- Motorised-Two Wheelers Liability Only Policy - Zone A Motor Insurance Certificate Cum Policy ScheduleDocument2 pagesMotorised-Two Wheelers Liability Only Policy - Zone A Motor Insurance Certificate Cum Policy ScheduleRevanth RajNo ratings yet
- Reliance Nippon Life Retire Smart: Complete Retirement PlanningDocument1 pageReliance Nippon Life Retire Smart: Complete Retirement PlanningAchche MitraNo ratings yet
- Total Reward SystemDocument10 pagesTotal Reward SystemFRANCIESNo ratings yet
- CS E CurrentDocument2 pagesCS E Current007shivangNo ratings yet