You might also like
- A Changing View On Sfas and Dairy: From Enemy To Friend: EditorialDocument2 pagesA Changing View On Sfas and Dairy: From Enemy To Friend: EditorialCaio Whitaker TosatoNo ratings yet
- Dietary Fats and Oils White PaperDocument25 pagesDietary Fats and Oils White Papermudassir qazalbashNo ratings yet
- Nutrients 10 01385Document16 pagesNutrients 10 01385Alex GutiérrezNo ratings yet
- Types of Dietary Fat and Risk of Coronary Heart Disease: A Critical ReviewDocument15 pagesTypes of Dietary Fat and Risk of Coronary Heart Disease: A Critical ReviewMegan KnightNo ratings yet
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
- Am J Clin Nutr 2015 Cespedes Ajcn.Document4 pagesAm J Clin Nutr 2015 Cespedes Ajcn.Jhon Sahatma SinagaNo ratings yet
- NIH Public Access: Artificial Sweeteners Produce The Counterintuitive Effect of Inducing Metabolic DerangementsDocument19 pagesNIH Public Access: Artificial Sweeteners Produce The Counterintuitive Effect of Inducing Metabolic DerangementsLuiggi D. Chambi MaidaNo ratings yet
- Siri-Tarino - Saturated Fat CHO e DCVDocument8 pagesSiri-Tarino - Saturated Fat CHO e DCVGracielaRecheNo ratings yet
- Review Article Effect of The Dietary Fat Quality On Insulin SensitivityDocument9 pagesReview Article Effect of The Dietary Fat Quality On Insulin SensitivityGilberto BicalhoNo ratings yet
- Articulo 45correctoDocument7 pagesArticulo 45correctoKarol Lizeth Paz ZuñigaNo ratings yet
- Nej M 199504133321512Document7 pagesNej M 199504133321512Sylvia IngridNo ratings yet
- Associations With Cardiometabolic Risk and Response To Weight LossDocument3 pagesAssociations With Cardiometabolic Risk and Response To Weight LossTeresa CuatecontziNo ratings yet
- Dietary Fat and Coronary Heart Disease - Summary of Evidence From Prospective Cohort and Random Is Ed Controlled TrialsDocument29 pagesDietary Fat and Coronary Heart Disease - Summary of Evidence From Prospective Cohort and Random Is Ed Controlled Trialsa_rogall7926No ratings yet
- Association of Dietary, Circulating, and Supplement Fatty Acids With Coronary RiskDocument7 pagesAssociation of Dietary, Circulating, and Supplement Fatty Acids With Coronary RiskVitor CordeiroNo ratings yet
- Decades of Diet Deception and the Spread of Non-Communicable Chronic DiseasesFrom EverandDecades of Diet Deception and the Spread of Non-Communicable Chronic DiseasesNo ratings yet
- Ultraprocessed Foods and Excess Heart Age Among Us AdultsDocument10 pagesUltraprocessed Foods and Excess Heart Age Among Us AdultsSaionara FranciscoNo ratings yet
- Busting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013Document2 pagesBusting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013jackjensen2852No ratings yet
- Stoke NutritionDocument14 pagesStoke Nutritionapi-150223943No ratings yet
- Caffeine Is Protective in Patients With Non-Alcoholic Fatty Liver DiseaseDocument7 pagesCaffeine Is Protective in Patients With Non-Alcoholic Fatty Liver DiseaseYelvi Novita RozaNo ratings yet
- Association of Dietary Fatty Acids With Coronary RiskDocument17 pagesAssociation of Dietary Fatty Acids With Coronary Riskubiktrash1492No ratings yet
- Stress-Associated Eating Leads To ObesityDocument2 pagesStress-Associated Eating Leads To ObesityYoga Agung PNo ratings yet
- Plasma Lipids: Optimal Levels for HealthFrom EverandPlasma Lipids: Optimal Levels for HealthAmerican Health FoundationNo ratings yet
- Polyunsaturated Fatty Acids, Specialized Pro-Resolving Mediators, and Targeting Inflammation Resolution in The Age of Precision NutritionDocument8 pagesPolyunsaturated Fatty Acids, Specialized Pro-Resolving Mediators, and Targeting Inflammation Resolution in The Age of Precision NutritionAndrés Felipe Gutiérrez RodríguezNo ratings yet
- Meta-Analysis in Research On Nutrition: To The EditorDocument2 pagesMeta-Analysis in Research On Nutrition: To The EditorLUISNo ratings yet
- ACS Guidelines PDFDocument38 pagesACS Guidelines PDFGabriel MateusNo ratings yet
- Journal of Hypertension and Management JHM 5 037Document10 pagesJournal of Hypertension and Management JHM 5 037reducdyantaNo ratings yet
- Dietary Saturated Fats and Their Food Sources in Relation To The RiskDocument8 pagesDietary Saturated Fats and Their Food Sources in Relation To The RiskJohn SammutNo ratings yet
- Obesidade Rio de JaneiroDocument7 pagesObesidade Rio de JaneiroarianeoliNo ratings yet
- Annotated BibliographyDocument4 pagesAnnotated Bibliographyapi-439027462No ratings yet
- Excess Protein Intake Relative To Fiber and Cardiovascular Events in Elderly Men With Chronic Kidney DiseaseDocument6 pagesExcess Protein Intake Relative To Fiber and Cardiovascular Events in Elderly Men With Chronic Kidney Diseaseluis Gomez VallejoNo ratings yet
- 营养:疾病预防和治疗Document12 pages营养:疾病预防和治疗张芬No ratings yet
- NutrientsDocument19 pagesNutrientsDadi SindhuNo ratings yet
- Nutrition and HypertensionDocument3 pagesNutrition and HypertensionKajee GrantNo ratings yet
- Nutrition and Prevention of Chronic-Degenerative Diseases: Sciencedirect SciencedirectDocument5 pagesNutrition and Prevention of Chronic-Degenerative Diseases: Sciencedirect SciencedirectJustNay 'nuna' Arief HusadaNo ratings yet
- Nutrients 05 02019Document9 pagesNutrients 05 02019FITYOURBODYNo ratings yet
- Low Carb ResearchDocument31 pagesLow Carb ResearchMozHeartNo ratings yet
- Dash Diet For Beginners - Lower Your Blood Pressure For Healthy Weight LossFrom EverandDash Diet For Beginners - Lower Your Blood Pressure For Healthy Weight LossNo ratings yet
- A Riview of Nutritional Factor in Hypertension ManagementDocument13 pagesA Riview of Nutritional Factor in Hypertension Managementprawira heroNo ratings yet
- 2016 Lacroix S Nutrition in CV RehabDocument7 pages2016 Lacroix S Nutrition in CV RehabHumamuddinNo ratings yet
- Am J Clin Nutr 2014 Chung Ajcn.114.086314Document17 pagesAm J Clin Nutr 2014 Chung Ajcn.114.086314Daniel Lee Eisenberg JacobsNo ratings yet
- Non Pharmacological Management of Hypertension - PMCDocument16 pagesNon Pharmacological Management of Hypertension - PMCBrian TaylorNo ratings yet
- Nutrients: The Environmental Regulation of Cardiovascular Gene ExpressionDocument6 pagesNutrients: The Environmental Regulation of Cardiovascular Gene ExpressionTrismegisteNo ratings yet
- Adherence To A Healthy Diet in Relation To Cardiovascular Incidence and Risk Markers Evidence From The Caerphilly Prospective StudyDocument14 pagesAdherence To A Healthy Diet in Relation To Cardiovascular Incidence and Risk Markers Evidence From The Caerphilly Prospective StudyRobet Agung wicaksonoNo ratings yet
- Pathophysiology of Obesity-Induced Health ComplicationsFrom EverandPathophysiology of Obesity-Induced Health ComplicationsParamjit S. TappiaNo ratings yet
- Prostaglandins, Leukotrienes and Essential Fatty AcidsDocument12 pagesProstaglandins, Leukotrienes and Essential Fatty AcidsNatália LopesNo ratings yet
- DASH DIET COOKBOOK: Nourishing Recipes to Lower Blood Pressure, Boost Heart Health, and Achieve Long-Term Well-Being (2024 Guide)From EverandDASH DIET COOKBOOK: Nourishing Recipes to Lower Blood Pressure, Boost Heart Health, and Achieve Long-Term Well-Being (2024 Guide)No ratings yet
- Research Open Access: Adi Lukas Kurniawan, Chien-Yeh Hsu, Hsiao-Hsien Rau, Li-Yin Lin and Jane C.-J. ChaoDocument11 pagesResearch Open Access: Adi Lukas Kurniawan, Chien-Yeh Hsu, Hsiao-Hsien Rau, Li-Yin Lin and Jane C.-J. ChaoLeonardo AzevedoNo ratings yet
- Nuts and Coronary Heart DiseaseDocument8 pagesNuts and Coronary Heart DiseasejparanotiNo ratings yet
- Dietary Fiber Intake and Glycemic Control: Coronary Artery Calcification in Type 1 Diabetes (CACTI) StudyDocument8 pagesDietary Fiber Intake and Glycemic Control: Coronary Artery Calcification in Type 1 Diabetes (CACTI) StudyLeonardo AzevedoNo ratings yet
- Ultra Processed Foods and Cardiovascular Diseases Poten - 2021 - Advances in NuDocument8 pagesUltra Processed Foods and Cardiovascular Diseases Poten - 2021 - Advances in NuMauricio RebolloNo ratings yet
- Shan. Association of Low-Carbohydrate and Low-Fat Diets With MortalityDocument20 pagesShan. Association of Low-Carbohydrate and Low-Fat Diets With MortalityMaria Julia Ogna EgeaNo ratings yet
- Term Paper 609Document10 pagesTerm Paper 609api-532399186No ratings yet
- Adherence To A Healthy Diet in Relation To Cardiovascular Incidence and Risk Markers - Evidence From The Caerphilly Prospective StudyDocument14 pagesAdherence To A Healthy Diet in Relation To Cardiovascular Incidence and Risk Markers - Evidence From The Caerphilly Prospective StudyXochitl PonceNo ratings yet
- Dean Ornish Mostly PlantsDocument2 pagesDean Ornish Mostly Plantsipman0100% (2)
- The Dash Diet: Lower Blood Pressure Lose Weight And Feel GreatFrom EverandThe Dash Diet: Lower Blood Pressure Lose Weight And Feel GreatNo ratings yet
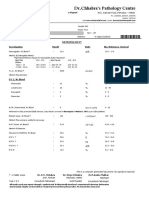
- DR - Chhabra's Pathology Centre: E-ReportDocument6 pagesDR - Chhabra's Pathology Centre: E-ReportHimanshu KalaNo ratings yet
- Modification of Fat and OilDocument18 pagesModification of Fat and OilPawan ShresthaNo ratings yet
- Drug Nutrient Depletions - Interactions ChartDocument2 pagesDrug Nutrient Depletions - Interactions ChartEygenia PapadpoulouNo ratings yet
- Excel Fro Payment LinkDocument7 pagesExcel Fro Payment LinkSanjay NadekarNo ratings yet
- CPT Code 99091 Alexander LDocument6 pagesCPT Code 99091 Alexander LBryan MorteraNo ratings yet
- Daftar Harga Qca Kimia Klinik Name of Products Catalog Packing Size Price Configuration Rp/kitDocument3 pagesDaftar Harga Qca Kimia Klinik Name of Products Catalog Packing Size Price Configuration Rp/kitKiki ItaNo ratings yet
- Total+Allowable+Error+Limits+Table+Example Rev20120725Document4 pagesTotal+Allowable+Error+Limits+Table+Example Rev20120725Meidina Siti HanifahNo ratings yet
- The Endocrine Pancreas: Regulation of Carbohydrate MetabolismDocument61 pagesThe Endocrine Pancreas: Regulation of Carbohydrate MetabolismNona AsolaNo ratings yet
- Lab Values 1Document30 pagesLab Values 1Ezekiel John GarciaNo ratings yet
- Primary Prevention of CVDDocument53 pagesPrimary Prevention of CVDYibeltal AssefaNo ratings yet
- The Latest News About AvocadosDocument4 pagesThe Latest News About Avocadosq wNo ratings yet
- Hapalan KardiovaskulerDocument3 pagesHapalan KardiovaskulerMithaNo ratings yet
- Effectof Educational Programfor Health Promoting LifestyleDocument11 pagesEffectof Educational Programfor Health Promoting LifestylePawan MishraNo ratings yet
- Clinical Chemistry 2Document65 pagesClinical Chemistry 2Jennifer BaluarteNo ratings yet
- 4 +basic+nutritionDocument71 pages4 +basic+nutritionJasmine CorreosNo ratings yet
- TDS-Liquid Margarine 105615 (8545 - 1)Document2 pagesTDS-Liquid Margarine 105615 (8545 - 1)Javier MoralesNo ratings yet
- 1 s2.0 S0955286317303868 MainDocument14 pages1 s2.0 S0955286317303868 MainAdib FraNo ratings yet
- T2DM PracticalGuide 20190718 FA Ebook2Document80 pagesT2DM PracticalGuide 20190718 FA Ebook2Nokoline HuNo ratings yet
- Co DR Rajagopal, 4Th Street Arokiya Nagar, NK Road, Near Eb Colony, Thanjavur, Tamilnadu.,613005Document16 pagesCo DR Rajagopal, 4Th Street Arokiya Nagar, NK Road, Near Eb Colony, Thanjavur, Tamilnadu.,613005Rahul GNo ratings yet
- Prioritization of ProblemsDocument3 pagesPrioritization of ProblemsBLABLEBLIBLOBLUUUNo ratings yet
- Https Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId 04IJ4X6CFze8WreRm1UotQDocument9 pagesHttps Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId 04IJ4X6CFze8WreRm1UotQvanitha vemulaNo ratings yet
- HDL DirectDocument2 pagesHDL DirectDinesh SreedharanNo ratings yet
- 8 Benefits of Mustard OilDocument10 pages8 Benefits of Mustard OilArshad Rezwan AbidNo ratings yet
- Lesson Plan - Cardiovascular DiseaseDocument5 pagesLesson Plan - Cardiovascular DiseaseNasimaNo ratings yet
- Doctors Testimonials For Gamma OryzanolDocument8 pagesDoctors Testimonials For Gamma OryzanolRAJESH ANNAMALAI ALNo ratings yet
- Cholesterol, The Mind, and The Brain - Harvard HealthDocument4 pagesCholesterol, The Mind, and The Brain - Harvard HealthArthur100% (2)
- J. Lipid Res.-1968-Glomset-155-67Document13 pagesJ. Lipid Res.-1968-Glomset-155-67Stefania CristinaNo ratings yet
- Diabetes Related CKD 2Document1 pageDiabetes Related CKD 2Jia-PeiWuNo ratings yet
- Tube Collection GuideDocument2 pagesTube Collection GuidePrincess JanNo ratings yet
- Time: 1 Hr. 30 Min. Total Marks: 60: Important InformationDocument9 pagesTime: 1 Hr. 30 Min. Total Marks: 60: Important Informationrishab KumarNo ratings yet