You might also like
- Social Media CalendarDocument3 pagesSocial Media CalendaryuricpNo ratings yet
- Digital MKTDocument27 pagesDigital MKTyuricpNo ratings yet
- MKT Your BusinessDocument36 pagesMKT Your BusinessyuricpNo ratings yet
- Omnichannel MKTDocument14 pagesOmnichannel MKTyuricpNo ratings yet
- Growth HackingDocument15 pagesGrowth HackingyuricpNo ratings yet
- Growth Hacking 03Document38 pagesGrowth Hacking 03yuricpNo ratings yet
- Methods of Digital MKTDocument21 pagesMethods of Digital MKTyuricpNo ratings yet
- Brainstorming 1203793603532275 2Document27 pagesBrainstorming 1203793603532275 2Jauhar JauharabadNo ratings yet
- Graphic Design Thinking by Ellen LuptonDocument19 pagesGraphic Design Thinking by Ellen LuptonyuricpNo ratings yet
- Spray DryerDocument9 pagesSpray DryeryuricpNo ratings yet
- Bueno y Vegano Feb19Document16 pagesBueno y Vegano Feb19yuricpNo ratings yet
- 7 Steps To Thinking Like A Genius PDFDocument12 pages7 Steps To Thinking Like A Genius PDFBelle Deleña100% (1)
- Coffee&Cocoa InternationalDocument6 pagesCoffee&Cocoa InternationalyuricpNo ratings yet
- Cafe Makisapa FoodsDocument2 pagesCafe Makisapa FoodsyuricpNo ratings yet
- Naturex Gingest PDFDocument5 pagesNaturex Gingest PDFyuricpNo ratings yet
- 7tips Successful Questionnaire DesignDocument12 pages7tips Successful Questionnaire DesignyuricpNo ratings yet
- Marketing Dynamics%2C Theory and Practice PDFDocument427 pagesMarketing Dynamics%2C Theory and Practice PDFyuricpNo ratings yet
- Business Model Canvas PosterDocument1 pageBusiness Model Canvas Posterosterwalder75% (4)
- Ensayo Design ThinkingDocument24 pagesEnsayo Design ThinkingyuricpNo ratings yet
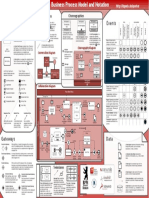
- Bpmn2 0 Poster enDocument1 pageBpmn2 0 Poster enTubora100% (1)
- Service With A Smile IdeateDocument14 pagesService With A Smile IdeateyuricpNo ratings yet
- Introduccion Al Business Canvas ModelDocument12 pagesIntroduccion Al Business Canvas ModelyuricpNo ratings yet
- CANVAS - Modelo de NegocioDocument22 pagesCANVAS - Modelo de NegocioyuricpNo ratings yet
- Libro Marketing RelacionalDocument164 pagesLibro Marketing RelacionalLorena Bustos Reinoso71% (7)
- 2 Digital Marketing Strategy Quirk Textbook 5Document14 pages2 Digital Marketing Strategy Quirk Textbook 5stanleyjebakumar2100% (1)
- Ficha Técnica Harina de LúcumaDocument4 pagesFicha Técnica Harina de LúcumayuricpNo ratings yet
- Ensayo Design Thinking PDFDocument24 pagesEnsayo Design Thinking PDFyuricpNo ratings yet
- Lean Canvas Creacion de Modelos de Negocio para StartupsDocument21 pagesLean Canvas Creacion de Modelos de Negocio para StartupsyuricpNo ratings yet
- Alimentacion Saludable PDFDocument78 pagesAlimentacion Saludable PDFyuricpNo ratings yet
- Air Travel by Generations Res LifeDocument44 pagesAir Travel by Generations Res LifeyuricpNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Deciphering Myanmar's Peace Process - A Reference Guide, 2013 ENGL.Document196 pagesDeciphering Myanmar's Peace Process - A Reference Guide, 2013 ENGL.Pugh Jutta100% (1)
- LTTE: A Revolution in Military AffairsDocument69 pagesLTTE: A Revolution in Military AffairseelamviewNo ratings yet
- Dignity, Values, Attitudes, and Person-Centred Care: Jo GallowayDocument14 pagesDignity, Values, Attitudes, and Person-Centred Care: Jo GallowayEdwin Mmaitsi Kodia100% (1)
- Carlos Whitlock Porter - Website ofDocument532 pagesCarlos Whitlock Porter - Website oftheoriginsofmidgardNo ratings yet
- Dealing With Difficult VolunteersDocument15 pagesDealing With Difficult VolunteersDan RoseNo ratings yet
- Healthy Relationships PDFDocument2 pagesHealthy Relationships PDFShawlar NaphewNo ratings yet
- Sarasota PD Internal InvestigationDocument69 pagesSarasota PD Internal Investigation10News WTSPNo ratings yet
- Character Traits and Jane EyreDocument2 pagesCharacter Traits and Jane EyreAhmed Abd El-hameed Ali50% (2)
- Monitoring and Enforcement of International Human Rights LawDocument2 pagesMonitoring and Enforcement of International Human Rights LawLee MatiasNo ratings yet
- Ya Lit Symposium Hand OutDocument24 pagesYa Lit Symposium Hand Outkelly jensenNo ratings yet
- Dew - Radio Spectrum Allocations in CanadaDocument1 pageDew - Radio Spectrum Allocations in CanadaHRCNo ratings yet
- Tolerance Unit PlanDocument8 pagesTolerance Unit PlanCaitlin MarieNo ratings yet
- Agrarian Law and Social Legislation SyllabusDocument2 pagesAgrarian Law and Social Legislation SyllabusAldous SisonNo ratings yet
- Hellstorm: The Death of NSDAP GermanyDocument6 pagesHellstorm: The Death of NSDAP GermanymediSin50% (2)
- Cruz Letter To DOJ - Cuties - FSVDocument1 pageCruz Letter To DOJ - Cuties - FSVLaw&CrimeNo ratings yet
- Implementation of Drug Abuse Resistance Education (DARE Program)Document3 pagesImplementation of Drug Abuse Resistance Education (DARE Program)Ellehctim BantigueNo ratings yet
- Mount Vernon DPW Supervisor Rudy Persaud Suspended Over Misconduct AllegationsDocument1 pageMount Vernon DPW Supervisor Rudy Persaud Suspended Over Misconduct AllegationsSamuel L. RiversNo ratings yet
- Peoria County Booking Sheet 10/26/14Document8 pagesPeoria County Booking Sheet 10/26/14Journal Star police documentsNo ratings yet
- UN SG's Statement On The Release of The Panel of Experts ReportDocument2 pagesUN SG's Statement On The Release of The Panel of Experts ReportSanjana HattotuwaNo ratings yet
- Charlatan D&D PDFDocument3 pagesCharlatan D&D PDFMarksdwarfNo ratings yet
- Unicef Study GuideDocument21 pagesUnicef Study Guideapi-229065565No ratings yet
- Revised Argumentative EssayDocument7 pagesRevised Argumentative Essayapi-316739257No ratings yet
- Peoria County Booking Sheet 04/19/15Document10 pagesPeoria County Booking Sheet 04/19/15Journal Star police documentsNo ratings yet
- Atty. Robert Aldrin B. Ortiz: Mr. Jose AbusadoDocument16 pagesAtty. Robert Aldrin B. Ortiz: Mr. Jose AbusadoRA OrtizNo ratings yet
- Abuse of Dominance: Indian ApproachDocument16 pagesAbuse of Dominance: Indian ApproachAnonymous 6lpK8Wb1h100% (1)
- UK Home Office: Cambridgeshire 2005Document31 pagesUK Home Office: Cambridgeshire 2005UK_HomeOfficeNo ratings yet
- Volume XXIII, Number 1 January & February 2008Document16 pagesVolume XXIII, Number 1 January & February 2008Ben LawlessNo ratings yet
- Republic Act No 7610 Child AbuseDocument16 pagesRepublic Act No 7610 Child AbuseJohnde MartinezNo ratings yet
- J S S 2Document18 pagesJ S S 2blessingnzeadibeNo ratings yet
- Complaint Responded To by DOTCDocument2 pagesComplaint Responded To by DOTCEmerson Kim LinesesNo ratings yet