You might also like
- Nec Hiv January-AidDocument4 pagesNec Hiv January-AiddocaisaNo ratings yet
- Natl Obj For HealthDocument9 pagesNatl Obj For HealthdocaisaNo ratings yet
- Natl Obj HealthDocument1 pageNatl Obj HealthdocaisaNo ratings yet
- The Philippine National Drug PolicyDocument7 pagesThe Philippine National Drug PolicydocaisaNo ratings yet
- HMODocument5 pagesHMOdocaisaNo ratings yet
- Hematol Oncol Clin North Am 2010 24 (1) 249-73Document25 pagesHematol Oncol Clin North Am 2010 24 (1) 249-73Paola Olate MelladoNo ratings yet
- Family As A Unit of Care IIDocument3 pagesFamily As A Unit of Care IIdocaisaNo ratings yet
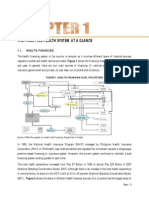
- The Philippine Health System at A GlanceDocument15 pagesThe Philippine Health System at A GlanceYL LYNo ratings yet
- Derm ManDocument7 pagesDerm Manmajid4uonlyNo ratings yet
- An Introduction To Medical Mycology: Definition of FungiDocument14 pagesAn Introduction To Medical Mycology: Definition of FungidocaisaNo ratings yet
- Blueprint FMDocument1 pageBlueprint FMdocaisaNo ratings yet
- National Objectives For HealthDocument15 pagesNational Objectives For Healthdocaisa0% (1)
- International Training Programmes 2012 13Document16 pagesInternational Training Programmes 2012 13docaisaNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument14 pagesIdiopathic Thrombocytopenic PurpuradocaisaNo ratings yet
- BLT 09 262Document12 pagesBLT 09 262docaisaNo ratings yet
- BLT 09 262Document12 pagesBLT 09 262docaisaNo ratings yet
- Diet Lifestyle Resource List 051013Document2 pagesDiet Lifestyle Resource List 051013docaisaNo ratings yet
- Child Has It P Entire BookletDocument8 pagesChild Has It P Entire BookletdocaisaNo ratings yet
- Hematology 2006 Nugent 97 103Document7 pagesHematology 2006 Nugent 97 103docaisaNo ratings yet
- Gout GuideDocument16 pagesGout GuidedocaisaNo ratings yet
- Health Book For TeachersDocument281 pagesHealth Book For TeachersRene H. Framcisco, MD100% (2)
- Itp Female LifecycleDocument30 pagesItp Female LifecycledocaisaNo ratings yet
- Blood 2011 Neunert 4190 207Document19 pagesBlood 2011 Neunert 4190 207docaisaNo ratings yet
- Cranial Nerves Mnemonics For Medical StudentsDocument2 pagesCranial Nerves Mnemonics For Medical StudentsdocaisaNo ratings yet
- Paypal Registration ProcessDocument18 pagesPaypal Registration ProcessdocaisaNo ratings yet
- The Number Coding SchemeDocument1 pageThe Number Coding SchemedocaisaNo ratings yet
- DengueDocument1 pageDenguedocaisaNo ratings yet
- History Taking Note CardDocument3 pagesHistory Taking Note Cardrmelendez001100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Contract ManagementDocument26 pagesContract ManagementGK TiwariNo ratings yet
- Devi Strotam PDFDocument9 pagesDevi Strotam PDFDiary Of A Wise ManNo ratings yet
- River: A Boon or A BaneDocument3 pagesRiver: A Boon or A BaneIJELS Research JournalNo ratings yet
- Application of Schiff Base Ligamd ComplexDocument7 pagesApplication of Schiff Base Ligamd Complexrajbharaths1094No ratings yet
- 332-Article Text-1279-1-10-20170327Document24 pages332-Article Text-1279-1-10-20170327Krisdayanti MendrofaNo ratings yet
- MMW SyllabusDocument13 pagesMMW SyllabusBien TecsonNo ratings yet
- Sampling TechniquesDocument96 pagesSampling Techniquessixteen liquidoNo ratings yet
- Stdy RhrupDocument331 pagesStdy RhrupSugesan SmileyNo ratings yet
- "The Sacrament of Confirmation": The Liturgical Institute S Hillenbrand Distinguished LectureDocument19 pages"The Sacrament of Confirmation": The Liturgical Institute S Hillenbrand Distinguished LectureVenitoNo ratings yet
- XM 301 StudDocument594 pagesXM 301 StudNarendar ReddyNo ratings yet
- Page 1 of 15 Vincent Balentino T. Batadlan RcrimDocument15 pagesPage 1 of 15 Vincent Balentino T. Batadlan RcrimJomarNo ratings yet
- Numerical Skills LectureDocument48 pagesNumerical Skills LecturezararNo ratings yet
- 2nd YearDocument46 pages2nd YearRajnish DeoNo ratings yet
- Test Bank For Marketing 12th Edition LambDocument24 pagesTest Bank For Marketing 12th Edition Lambangelascottaxgeqwcnmy100% (39)
- Say. - .: Examining Contemporary: Tom Daley's Something I Want To Celebrity, Identity and SexualityDocument5 pagesSay. - .: Examining Contemporary: Tom Daley's Something I Want To Celebrity, Identity and SexualityKen Bruce-Barba TabuenaNo ratings yet
- 5.1 ReteachDocument2 pages5.1 ReteachCarlos Pastrana0% (1)
- G8DDocument61 pagesG8Dvivek1312100% (1)
- Data ListDocument239 pagesData Listpriyanka chithran100% (1)
- Construction Quality Management 47 PDFDocument47 pagesConstruction Quality Management 47 PDFCarl WilliamsNo ratings yet
- Syntax Made Easy (Roberta D'Alessandro)Document23 pagesSyntax Made Easy (Roberta D'Alessandro)John DoeNo ratings yet
- Exercises 2Document7 pagesExercises 2Taseen Junnat SeenNo ratings yet
- Manila Jocky Club Vs CADocument20 pagesManila Jocky Club Vs CAryusuki takahashiNo ratings yet
- Radiology Developing Technique ChartsDocument4 pagesRadiology Developing Technique ChartsVarghese NellimoottilNo ratings yet
- Mambisas. Rebel Women in Nineteenth-Century Cuba (Libro Digital)Document201 pagesMambisas. Rebel Women in Nineteenth-Century Cuba (Libro Digital)SusanaNo ratings yet
- Experimental Nucleonics PDFDocument1 pageExperimental Nucleonics PDFEricNo ratings yet
- Principles and Methods of Effective TeachingDocument5 pagesPrinciples and Methods of Effective TeachingerikaNo ratings yet
- Dwnload Full Social Psychology 4th Edition Gilovich Test Bank PDFDocument35 pagesDwnload Full Social Psychology 4th Edition Gilovich Test Bank PDFalilonghidotardlyq71i7f100% (8)
- Navneet Publications India Limited HardDocument34 pagesNavneet Publications India Limited Harddyumna100% (1)
- 6 Money SupplyDocument6 pages6 Money SupplySaroj LamichhaneNo ratings yet
- Fossils (DK Smithsonian Handbook) by DKDocument320 pagesFossils (DK Smithsonian Handbook) by DKAnthony Mello71% (7)