You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Smile Esthetics in Othtodontics - Review of LiteratureDocument5 pagesSmile Esthetics in Othtodontics - Review of LiteratureLuis HerreraNo ratings yet
- Clinical Photography in An Orthodontic Practice Environment Part 1Document6 pagesClinical Photography in An Orthodontic Practice Environment Part 1Luis HerreraNo ratings yet
- Extraction Treatment, Part 2: Guidelines For Making The Extraction DecisionDocument7 pagesExtraction Treatment, Part 2: Guidelines For Making The Extraction DecisionLuis HerreraNo ratings yet
- Cephalometric Norms From Posteroanterior Ricketts' Cephalograms From Hispanic American Peruvian Non Adult PatientsDocument8 pagesCephalometric Norms From Posteroanterior Ricketts' Cephalograms From Hispanic American Peruvian Non Adult PatientsLuis HerreraNo ratings yet
- Ajodo Clase II-2 2018Document9 pagesAjodo Clase II-2 2018Luis HerreraNo ratings yet
- 2003.john H. Warford JR - Prediction of Maxillary Canine Impaction UsingDocument5 pages2003.john H. Warford JR - Prediction of Maxillary Canine Impaction UsingLuis HerreraNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Acido TranexamicoDocument8 pagesAcido TranexamicoVianey GarciaVillegasNo ratings yet
- Form 6 Revised 2022Document2 pagesForm 6 Revised 2022Angelo AlcantaraNo ratings yet
- CTO GuideDocument14 pagesCTO GuideTeodor BicaNo ratings yet
- Atlas of Large Animal SurgeryDocument147 pagesAtlas of Large Animal SurgeryAbdallah Fathi100% (4)
- Chakra Var Thy 2018Document15 pagesChakra Var Thy 2018Vlady78No ratings yet
- DR Dhara Tandel: Contact NB - 07960427298 Email - GMC NB - 7693484Document4 pagesDR Dhara Tandel: Contact NB - 07960427298 Email - GMC NB - 7693484Dhara ParmarNo ratings yet
- Biliary Tract Surgery 2008, Vol.88, Issues 6Document292 pagesBiliary Tract Surgery 2008, Vol.88, Issues 6Barbero JuanNo ratings yet
- Mobile Phones - Know Their Impact On Speech & Communication! - by Dr. Farheen Saif - LybrateDocument48 pagesMobile Phones - Know Their Impact On Speech & Communication! - by Dr. Farheen Saif - LybrateJayesh IsamaliyaNo ratings yet
- DR Surya SynopsisDocument29 pagesDR Surya SynopsisPrashant TiwariNo ratings yet
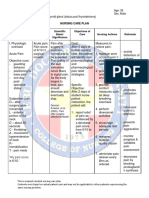
- Sample Nursing Care PlanDocument1 pageSample Nursing Care PlanQuiannë Delos ReyesNo ratings yet
- Coronectomy A Surgical Option For Impacted Third Molars in Close Proximity To TheDocument25 pagesCoronectomy A Surgical Option For Impacted Third Molars in Close Proximity To TheAndi Askandar AminNo ratings yet
- The Complete Orthopaedic Examination of Patients With Injuries and Diseases of The Locomotor SystemDocument35 pagesThe Complete Orthopaedic Examination of Patients With Injuries and Diseases of The Locomotor SystemAndreea DanielaNo ratings yet
- Fluid Management in Perioperative and Critically Ill Patients - Acute and Critical Care PDFDocument11 pagesFluid Management in Perioperative and Critically Ill Patients - Acute and Critical Care PDFMaria Siachoque JaraNo ratings yet
- Exercise 7 - Suture Patterns For Soft Tissues, Hollow Organs and TendonsDocument5 pagesExercise 7 - Suture Patterns For Soft Tissues, Hollow Organs and TendonsJhayar SarionNo ratings yet
- Archives PDFDocument344 pagesArchives PDFchaib meriemNo ratings yet
- Geniculate Artery Embolization: Role in Knee Hemarthrosis and OsteoarthritisDocument13 pagesGeniculate Artery Embolization: Role in Knee Hemarthrosis and Osteoarthritis李冠No ratings yet
- Sublingual Sialocele in A Cat: Jean Bassanino, Sophie Palierne, Margaux Blondel and Brice S ReynoldsDocument5 pagesSublingual Sialocele in A Cat: Jean Bassanino, Sophie Palierne, Margaux Blondel and Brice S ReynoldsTarsilaRibeiroMaiaNo ratings yet
- NRG 304 Return Demonstration - Wound CareDocument8 pagesNRG 304 Return Demonstration - Wound CareEmmy Flor ValmoriaNo ratings yet
- Tatalaksana Katarak Komplikata Yang Disebabkan Oleh Uveitis - Ericka Febriyanti Pratama Putri 1Document14 pagesTatalaksana Katarak Komplikata Yang Disebabkan Oleh Uveitis - Ericka Febriyanti Pratama Putri 1Cynthia Isra MandahutaNo ratings yet
- Dokumen - Pub - Hadzics Textbook of Regional Anesthesia and Acute Pain Management Self Assessment and Review 1nbsped 9781260142716 126014271x 9781260142709 1260142701Document449 pagesDokumen - Pub - Hadzics Textbook of Regional Anesthesia and Acute Pain Management Self Assessment and Review 1nbsped 9781260142716 126014271x 9781260142709 1260142701Cinthia Gonzalez Nunez100% (5)
- Tugas Jurnal Nerve IschiadicusDocument4 pagesTugas Jurnal Nerve IschiadicusrahmawatiNo ratings yet
- Recognized Ho So ListDocument77 pagesRecognized Ho So Listdp663668No ratings yet
- Assignment On CT Scan: Submitted To, Mrs - Regi Philip Professor Hod of MSN, Sjcon, AnchalDocument6 pagesAssignment On CT Scan: Submitted To, Mrs - Regi Philip Professor Hod of MSN, Sjcon, AnchalAxsa AlexNo ratings yet
- CC Product Catalog 022223Document55 pagesCC Product Catalog 022223Huong NguyenNo ratings yet
- 6255 24879 1 PBDocument2 pages6255 24879 1 PBSyafatesia nicky pratiwiNo ratings yet
- Cleft Lip 2021Document52 pagesCleft Lip 2021Mohammad AyyashNo ratings yet
- Gerard A Malanga - Scott Nadler - Whiplash-Hanley & Belfus (2002) PDFDocument453 pagesGerard A Malanga - Scott Nadler - Whiplash-Hanley & Belfus (2002) PDFNu'man 'Zeus' AnggaraNo ratings yet
- Full Download Book Surgery Pretest Self Assessment and Review 14E PDFDocument41 pagesFull Download Book Surgery Pretest Self Assessment and Review 14E PDFemilio.elliott723100% (16)
- Head To Head: Should All Advertising of Cosmetic Surgery Be Banned? YesDocument2 pagesHead To Head: Should All Advertising of Cosmetic Surgery Be Banned? YesLIM YIN SHENG / UPMNo ratings yet
- 1 PBDocument8 pages1 PBMahathir Harry PermanaNo ratings yet