You might also like
- Take Charge of Your Fertility: A Step by Step Guide to Making Babies, Including Getting Pregnant Naturally, Preventing Miscarriage and Improving Your Chances in IVFFrom EverandTake Charge of Your Fertility: A Step by Step Guide to Making Babies, Including Getting Pregnant Naturally, Preventing Miscarriage and Improving Your Chances in IVFRating: 3 out of 5 stars3/5 (1)
- Abortion: MiscarriageDocument11 pagesAbortion: MiscarriageTotep ReyesNo ratings yet
- Holding Hands Through IVF; Supporting Your Fertility Journey With Complementary TherapiesFrom EverandHolding Hands Through IVF; Supporting Your Fertility Journey With Complementary TherapiesNo ratings yet
- Pregnancy Choices: Raising The Baby, Adoption, and AbortionDocument3 pagesPregnancy Choices: Raising The Baby, Adoption, and AbortionSebastian Sandoval ChavarroNo ratings yet
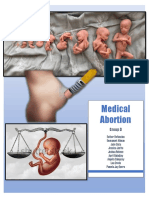
- Medical AbortionDocument11 pagesMedical AbortionEsther RefuncionNo ratings yet
- Abortion - Topic OverviewDocument4 pagesAbortion - Topic OverviewTesy Sii SleeperNo ratings yet
- 02 85 Medical Management of A MiscarriageDocument16 pages02 85 Medical Management of A MiscarriageBrianJakeDelRosarioNo ratings yet
- Abortion - NHSDocument1 pageAbortion - NHSElla VladNo ratings yet
- Family Planning Methods GuideDocument32 pagesFamily Planning Methods GuideCarson BirthNo ratings yet
- Self-Managed Medical AbortionDocument2 pagesSelf-Managed Medical AbortionGerri SantoroNo ratings yet
- Biology Investigation 2 PDFDocument15 pagesBiology Investigation 2 PDFNoella RalteNo ratings yet
- Medical Versus Surgical Abortion - Patient Education - UCSF Medical CenterDocument3 pagesMedical Versus Surgical Abortion - Patient Education - UCSF Medical CenterSubhashish ChowdhuryNo ratings yet
- Caesarean Section: Understanding NICE GuidanceDocument20 pagesCaesarean Section: Understanding NICE GuidanceAtika RestuningsihNo ratings yet
- Early MiscarriageretrjytkuyiulDocument6 pagesEarly MiscarriageretrjytkuyiulMuhammed BarznjiNo ratings yet
- Infertility-An Overview Booklet2Document20 pagesInfertility-An Overview Booklet2Sakshi SinghNo ratings yet
- How to do an abortion in 10 stepsDocument5 pagesHow to do an abortion in 10 stepsShien Brojas OropesaNo ratings yet
- Ready For PregnancyDocument9 pagesReady For PregnancylookloNo ratings yet
- Final Resech PaperDocument9 pagesFinal Resech Paperapi-459387406No ratings yet
- Pregnancy Abortion: Unloading A Loaded IssueDocument6 pagesPregnancy Abortion: Unloading A Loaded IssueRigorMortizNo ratings yet
- TextDocument2 pagesTextlydialoocuckooNo ratings yet
- Oumo JosephDocument30 pagesOumo JosephRonald SserunjogiNo ratings yet
- Iud Insertion Removal in ClinicDocument6 pagesIud Insertion Removal in ClinicBhavna SapreNo ratings yet
- Infertility An Overview Booklet PDFDocument24 pagesInfertility An Overview Booklet PDFSara Al-FerkhNo ratings yet
- About Abortion:: Please E-Mail UsDocument9 pagesAbout Abortion:: Please E-Mail UsNeric Ico MagleoNo ratings yet
- What Is A Miscarriage and Abortion Similarities and DifferencesDocument9 pagesWhat Is A Miscarriage and Abortion Similarities and DifferencesOvais HussaiinNo ratings yet
- Vte Prepregnancy CounselingDocument2 pagesVte Prepregnancy CounselingSana LodhiNo ratings yet
- Case Study K.WDocument3 pagesCase Study K.WSharon Williams50% (2)
- After Miscarriage 250320Document3 pagesAfter Miscarriage 250320Putu Gede WidyatamaNo ratings yet
- 4 _ PRETERM BIRTHDocument13 pages4 _ PRETERM BIRTHsaeed hasan saeedNo ratings yet
- Your Antenatal Care - NHS PDFDocument1 pageYour Antenatal Care - NHS PDFS SNo ratings yet
- CF433 Medical Management of An Ectopic Pregnancy Using MethotrexateDocument11 pagesCF433 Medical Management of An Ectopic Pregnancy Using MethotrexateponekNo ratings yet
- Importance of Prenatal Care Checkups (40Document56 pagesImportance of Prenatal Care Checkups (40Al YsSa Ricafort MillabasNo ratings yet
- Antenatal Care What Is Meant by Antenatal Care?Document6 pagesAntenatal Care What Is Meant by Antenatal Care?Syed Haseeb AhmedNo ratings yet
- When To Take A Pregnancy Test Options, Cost andDocument1 pageWhen To Take A Pregnancy Test Options, Cost andOyedele OluwaseunNo ratings yet
- Marquez - Case Study 120Document4 pagesMarquez - Case Study 120Caren Marquez100% (1)
- Pregnancy OptionsDocument116 pagesPregnancy OptionsBharti CartesNo ratings yet
- Prenatal CareDocument27 pagesPrenatal CareMae PalacioNo ratings yet
- Contraceptives Written ReportDocument17 pagesContraceptives Written ReportChristine GuibaoNo ratings yet
- Use of methotrexate to treat pregnancy of unknown location and ectopic pregnancy_NBT002435Document12 pagesUse of methotrexate to treat pregnancy of unknown location and ectopic pregnancy_NBT002435autokucamatijevic1No ratings yet
- Different Methods of Family PlanningDocument8 pagesDifferent Methods of Family PlanningFamela LauzonNo ratings yet
- Everything You Need to Know About Prenatal CareDocument5 pagesEverything You Need to Know About Prenatal Carelaura fernandiaNo ratings yet
- Family Planning and HormonalDocument44 pagesFamily Planning and HormonalAbdinafa Mahamud DiriyeNo ratings yet
- Mandatory Language Birth PlanDocument5 pagesMandatory Language Birth PlanWalter WallabyNo ratings yet
- CIIC AbortionPillDocument2 pagesCIIC AbortionPillAngelicia RobertsonNo ratings yet
- Going All The Way: Can I Have Sex and Be Sure I Won'T Get Pregnant?Document2 pagesGoing All The Way: Can I Have Sex and Be Sure I Won'T Get Pregnant?DebbieNo ratings yet
- Step 1 To Whom Surrogacy Is Advised?Document5 pagesStep 1 To Whom Surrogacy Is Advised?Shrikant DarneNo ratings yet
- Sex 3Document11 pagesSex 3Abhijit BNo ratings yet
- Methotrexate: Department of GynaecologyDocument8 pagesMethotrexate: Department of GynaecologyFakhrul IslamNo ratings yet
- ContraceptionDocument155 pagesContraceptionAprilyn Abellera DifuntorumNo ratings yet
- Family PlanningDocument6 pagesFamily PlanningDhanica Yvonne ReymonteNo ratings yet
- AbortionDocument4 pagesAbortionsuubae41No ratings yet
- Questions: To Ask Your DoctorsDocument15 pagesQuestions: To Ask Your DoctorsAvik GhoshNo ratings yet
- ContraceptionDocument156 pagesContraceptionLorenn DacpanoNo ratings yet
- The Combined Oral Contraceptive Pill: Fact SheetDocument3 pagesThe Combined Oral Contraceptive Pill: Fact SheetTommy Prima TarunaNo ratings yet
- Ovulation Induction and Intra Uterine InseminationDocument4 pagesOvulation Induction and Intra Uterine InseminationmasdipoNo ratings yet
- Pi Ectopic Pregnancy Mar20Document9 pagesPi Ectopic Pregnancy Mar20Aziza TahanyNo ratings yet
- Abhpa Baby BookDocument32 pagesAbhpa Baby BookAnca BiancaNo ratings yet
- Korea DeliveriesDocument4 pagesKorea Deliveriesseri ChannelNo ratings yet
- ART Handbook: A Step by Step GuideDocument25 pagesART Handbook: A Step by Step GuideNilesh SuvagiyaNo ratings yet
- MHRA Always Read Leaflet 2005Document173 pagesMHRA Always Read Leaflet 2005Sandeep_Bellap_5543No ratings yet
- Keto SisDocument5 pagesKeto SisSandeep_Bellap_5543No ratings yet
- Mitsubishi Electric Group Conduct GuidelinesDocument15 pagesMitsubishi Electric Group Conduct GuidelinesSandeep_Bellap_5543No ratings yet
- Now or Never - Patient LeafletDocument6 pagesNow or Never - Patient LeafletSandeep_Bellap_5543No ratings yet
- East Vs West Ed1Document14 pagesEast Vs West Ed1Ray NanNo ratings yet
- LAC - Air Oil Cooler With AC Motor For Industrial Use - HY10-6001.UKDocument12 pagesLAC - Air Oil Cooler With AC Motor For Industrial Use - HY10-6001.UKSandeep_Bellap_5543No ratings yet
- Prescribing Guidance - PDF 59055247Document11 pagesPrescribing Guidance - PDF 59055247Sandeep_Bellap_5543No ratings yet
- Saying Sorry - LeafletDocument4 pagesSaying Sorry - LeafletSandeep_Bellap_5543No ratings yet
- Con 1464324364725Document4 pagesCon 1464324364725Sandeep_Bellap_5543No ratings yet
- Business Plan TemplateDocument15 pagesBusiness Plan TemplateSandeep_Bellap_5543No ratings yet
- Falsifiedmedicines Leaflet enDocument2 pagesFalsifiedmedicines Leaflet enSandeep_Bellap_5543No ratings yet
- Kokate Forensic Pharmacy PDFDocument201 pagesKokate Forensic Pharmacy PDFSouvik Saha100% (2)
- vepBusinessPlanOutline PDFDocument20 pagesvepBusinessPlanOutline PDFMark John Christian LumindasNo ratings yet
- Best Way of Investment With HindiDocument33 pagesBest Way of Investment With HindiSandeep_Bellap_5543No ratings yet
- Child Sexual AbuseDocument85 pagesChild Sexual AbuseSandeep_Bellap_5543No ratings yet
- Wf338 - Manual Lavadora SamsumgDocument60 pagesWf338 - Manual Lavadora Samsumgjorge_chaparro_1No ratings yet
- Shri Swami Samartha (Akkalkot) - BiographyDocument243 pagesShri Swami Samartha (Akkalkot) - BiographySB Dev85% (20)
- Kokate Forensic Pharmacy PDFDocument201 pagesKokate Forensic Pharmacy PDFSouvik Saha100% (2)
- Nexphase User GuideDocument48 pagesNexphase User GuideSandeep_Bellap_554369% (13)
- Discovery India NehruDocument577 pagesDiscovery India NehrupreetihNo ratings yet
- Nay Nay's PrivateDocument1,203 pagesNay Nay's Privatemriley@gmail.comNo ratings yet
- Dispensing Contractors - Issue 6 (V1) 12.01.2012Document6 pagesDispensing Contractors - Issue 6 (V1) 12.01.2012Sandeep_Bellap_5543No ratings yet
- Listening Script 1Document9 pagesListening Script 1Babi BeloNo ratings yet
- BHLMP-Form1 B-Ver2 1Document17 pagesBHLMP-Form1 B-Ver2 1Christine BeltranNo ratings yet
- PathologyDocument31 pagesPathologyStudy Usmle100% (1)
- Teacher Training on Menstrual HealthDocument12 pagesTeacher Training on Menstrual HealthJoseph ChakmaNo ratings yet
- Community Health Nursing Part 1Document24 pagesCommunity Health Nursing Part 1iko552000100% (3)
- Intraoperative Fluid ManagementDocument15 pagesIntraoperative Fluid ManagementMirela Marina BlajNo ratings yet
- HeFRA APPLICATION FORM V7.0 FREEDocument10 pagesHeFRA APPLICATION FORM V7.0 FREEMichael BusiaNo ratings yet
- MRCP Exam ResultDocument2 pagesMRCP Exam ResultOmeca Mymensingh100% (1)
- MetodeDocument17 pagesMetodeiuliaschiporNo ratings yet
- 008 Uk Geoff Knight Riva Star v2 1Document2 pages008 Uk Geoff Knight Riva Star v2 1api-240710651No ratings yet
- Haaga 1Document1,216 pagesHaaga 1Anca Mehedințu100% (1)
- Regional Anesthesia: Brachial Plexus BlockDocument77 pagesRegional Anesthesia: Brachial Plexus BlockTerefe AlemayehuNo ratings yet
- Adnexal MassDocument28 pagesAdnexal MassJuan P. RuedaNo ratings yet
- Endoscopic Tumour Surgery - Current Limits and Future PossibilitiesDocument4 pagesEndoscopic Tumour Surgery - Current Limits and Future PossibilitiesIliasa IliasNo ratings yet
- Clinical Case Study-Lung CancerDocument14 pagesClinical Case Study-Lung Cancerapi-299403846100% (1)
- List of CGHS Hospital As On 20.07.2023Document3 pagesList of CGHS Hospital As On 20.07.2023কৌশিক ঘোষNo ratings yet
- Midwifery KitDocument3 pagesMidwifery KitRitzel CreusNo ratings yet
- Orthodontic Treatment in The Management of Cleft Lip and PalateDocument13 pagesOrthodontic Treatment in The Management of Cleft Lip and PalatecareNo ratings yet
- Bryan James G. Punzal: CurettageDocument2 pagesBryan James G. Punzal: Curettagehob_ioqeq0% (1)
- Christa Maki Letter of Recommednation 4Document2 pagesChrista Maki Letter of Recommednation 4api-491578633No ratings yet
- Walrus Syndrome in Three English Bulldog Puppies: Case ReportDocument1 pageWalrus Syndrome in Three English Bulldog Puppies: Case ReportJuanita AristizabalNo ratings yet
- Midwives' Intrapartum Monitoring Process and Management Resulting in Emergency Referrals in TanzaniaDocument11 pagesMidwives' Intrapartum Monitoring Process and Management Resulting in Emergency Referrals in TanzaniaAdhiw AmanNo ratings yet
- Corneal Degenerations and DystrophiesDocument12 pagesCorneal Degenerations and DystrophiesSuleman MuhammadNo ratings yet
- YurkonresumeDocument2 pagesYurkonresumeapi-317112295No ratings yet
- Divine Intervention Episode 36 Usmle OphthalmologyDocument15 pagesDivine Intervention Episode 36 Usmle OphthalmologySwisskelly1No ratings yet
- Dental BooklistDocument14 pagesDental Booklistالمكتبة المليونيةNo ratings yet
- Symphonic 2023Document6 pagesSymphonic 2023Muthya Aulina FahriyanNo ratings yet
- Surgical Drains. What The Resident Needs To KnowDocument8 pagesSurgical Drains. What The Resident Needs To Knowginoahnna33No ratings yet
- Name:Putri Al Zahra Prodi:S1 Keperawatan Semester: 2: Tugas Individu B. InggrisDocument6 pagesName:Putri Al Zahra Prodi:S1 Keperawatan Semester: 2: Tugas Individu B. InggrisPutri Al ZahraNo ratings yet
- Endocrinology Take Home ExamDocument7 pagesEndocrinology Take Home ExamRenz L. SalumbreNo ratings yet
- Signs and Symptoms of Neonatal PneumoniaDocument4 pagesSigns and Symptoms of Neonatal PneumoniaMäc LäntinNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)