You might also like
- CDC Misinformation EmailsDocument76 pagesCDC Misinformation EmailsZerohedge Janitor100% (2)
- Management of Patient With CancerDocument52 pagesManagement of Patient With CancerAru VermaNo ratings yet
- RecruitmentDocument20 pagesRecruitmentpinoybsn26No ratings yet
- Maternity Nursing Course Outline - Clinical PDFDocument24 pagesMaternity Nursing Course Outline - Clinical PDFAshraf NoriNo ratings yet
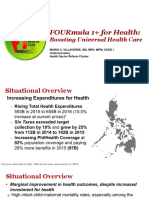
- 4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoDocument12 pages4 FOURmula 1 For Health Boosting Universal Health Care by DR Beverly HoJanella DandanNo ratings yet
- Mental Health Nursing Case StudyDocument10 pagesMental Health Nursing Case Studyapi-403093734No ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Patient Care Plan 1Document3 pagesPatient Care Plan 1api-311242332No ratings yet
- Chronic Suppurative Otitis MediaDocument14 pagesChronic Suppurative Otitis MediaIkhsan100% (1)
- Wafa Obgyn Smle2021Document146 pagesWafa Obgyn Smle2021Amal100% (1)
- Immunization ScheduleDocument18 pagesImmunization Scheduledr parveen bathlaNo ratings yet
- Medication Adherence Questionnaire (MAQ) : ARMS ScaleDocument4 pagesMedication Adherence Questionnaire (MAQ) : ARMS ScaleEnesaHodžićNo ratings yet
- Emergency CodesDocument23 pagesEmergency CodesJennifer B. GarciaNo ratings yet
- IFUk en 311220 04Document12 pagesIFUk en 311220 04Trunggana AbdulNo ratings yet
- B.sc. Nursing Syllabus.Document120 pagesB.sc. Nursing Syllabus.Asif AliNo ratings yet
- Chapter 24: Communication Communication and Nursing PracticeDocument4 pagesChapter 24: Communication Communication and Nursing PracticejoanneNo ratings yet
- Epidemiological MethodsDocument22 pagesEpidemiological MethodsDolly Dutta0% (1)
- TetanusDocument32 pagesTetanusVinotheran MichaelNo ratings yet
- Oet Sample SpeakingDocument84 pagesOet Sample Speakingissac jetto100% (5)
- Ppra Mdro SurgeryDocument55 pagesPpra Mdro SurgeryDimas ErlanggaNo ratings yet
- Natural History of DiseaseDocument31 pagesNatural History of Diseasegabo dasNo ratings yet
- Epi ReviewerDocument4 pagesEpi ReviewerHannah VueltaNo ratings yet
- Diphtheria: About The DiseaseDocument18 pagesDiphtheria: About The DiseaseJesse EstradaNo ratings yet
- DiphtheriaDocument49 pagesDiphtheriasultanNo ratings yet
- Week 2 Evolution of NursingDocument73 pagesWeek 2 Evolution of NursingAna PimentelNo ratings yet
- Anatomy & Physiology: Acute Otitis MediaDocument7 pagesAnatomy & Physiology: Acute Otitis MediaAbigael Patricia GutierrezNo ratings yet
- Otitis Media Diagnosis and TreatmentDocument19 pagesOtitis Media Diagnosis and TreatmentreyhanrrNo ratings yet
- Pediatric Acute Anemia PDFDocument6 pagesPediatric Acute Anemia PDFpurwanto nugrohoNo ratings yet
- DiphtheriaDocument18 pagesDiphtheriaShishir ShresthaNo ratings yet
- AuditionDocument35 pagesAuditionBam SeñeresNo ratings yet
- Otitis Media Report 130504Document399 pagesOtitis Media Report 130504Yanna RizkiaNo ratings yet
- Use of Sedation in Palliative CareDocument13 pagesUse of Sedation in Palliative Careuriel_rojas_41No ratings yet
- Liverpool Care Pathway PDFDocument63 pagesLiverpool Care Pathway PDFBryan DorosanNo ratings yet
- AEFIDocument24 pagesAEFIadiNo ratings yet
- Human Becoming TheoryDocument7 pagesHuman Becoming TheoryDelvianaNo ratings yet
- Bioethics LectureDocument40 pagesBioethics LecturejeshemaNo ratings yet
- Patient Safety and Quality Care MovementDocument9 pagesPatient Safety and Quality Care Movementapi-300362983No ratings yet
- Communicable Disease SudanDocument130 pagesCommunicable Disease Sudansida200100% (1)
- Patient SafetyDocument102 pagesPatient SafetyAlain CheryNo ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
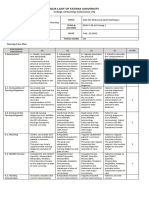
- NCP Rubric Sec 16 Group 1Document2 pagesNCP Rubric Sec 16 Group 1HILARY MAE MARINNo ratings yet
- History of Community Health NursingDocument35 pagesHistory of Community Health NursingAgung setiawan100% (1)
- Hea LTH Edu Cati OnDocument10 pagesHea LTH Edu Cati Onmaria erika100% (1)
- CHN Health PromotionDocument7 pagesCHN Health PromotionNareeza AbdullaNo ratings yet
- Non Communicable DiseaseDocument13 pagesNon Communicable DiseaseClancy Anne Garcia Naval100% (1)
- Monitoring Intake & OutputDocument16 pagesMonitoring Intake & OutputSalome RahimNo ratings yet
- Nur 330 - Health Promotion ProjectDocument12 pagesNur 330 - Health Promotion Projectapi-375928224No ratings yet
- Otitis MediaDocument6 pagesOtitis MediaririNo ratings yet
- Updated NCM 103.1 NCP Making ActivityDocument2 pagesUpdated NCM 103.1 NCP Making ActivityCyrillNo ratings yet
- Communicable DiseasesDocument24 pagesCommunicable DiseasesJanus de LeonNo ratings yet
- Reproductive Tract InfectionDocument48 pagesReproductive Tract InfectionSampriti Roy100% (1)
- EBOLADocument4 pagesEBOLAwawa3385No ratings yet
- The WHO Health Promotion Glossary PDFDocument17 pagesThe WHO Health Promotion Glossary PDFfirda FibrilaNo ratings yet
- SOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticDocument5 pagesSOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticvidyahamzahNo ratings yet
- Essential BSNDocument5 pagesEssential BSNpurplestainedNo ratings yet
- Infection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementDocument125 pagesInfection Prevention (Including Hiv), Standard Precaution, Bio Waste ManagementZhu Chen ChuanNo ratings yet
- NCM108 Health Care Ethics Course OutlineDocument5 pagesNCM108 Health Care Ethics Course Outlinemirai desuNo ratings yet
- Running Head: Pico Question: Aseptic Technique 1Document10 pagesRunning Head: Pico Question: Aseptic Technique 1api-253019091No ratings yet
- 2014-02-17 Acid Base Physiology and ABG Interpretation PDFDocument149 pages2014-02-17 Acid Base Physiology and ABG Interpretation PDFIva Dewi Permata PhilyNo ratings yet
- Pediatric Nursing 1الجزء الأولDocument291 pagesPediatric Nursing 1الجزء الأولAhmed Elryah0% (1)
- Bronchiolitis ManagementDocument21 pagesBronchiolitis ManagementboojectNo ratings yet
- Sexually Transmitted DiseasesDocument5 pagesSexually Transmitted Diseasesreghpineda28No ratings yet
- Nursing ProcessDocument62 pagesNursing ProcessplethoraldorkNo ratings yet
- Patient Safety: What Should We Be Trying To Communicate?Document32 pagesPatient Safety: What Should We Be Trying To Communicate?cicaklomenNo ratings yet
- British Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyDocument6 pagesBritish Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyPriscilla CarmiolNo ratings yet
- NHS LA - Duty of Candour 2014 - SlidesDocument10 pagesNHS LA - Duty of Candour 2014 - SlidesAgnieszka WaligóraNo ratings yet
- Child CPR: Skills Testing ChecklistDocument3 pagesChild CPR: Skills Testing ChecklistTravis TravoltaNo ratings yet
- AsqeDocument11 pagesAsqebrigde_xNo ratings yet
- Xodo Document - Periprocedural - Anticoagulation - GuidelineDocument16 pagesXodo Document - Periprocedural - Anticoagulation - Guidelinebrigde_xNo ratings yet
- Trombocitopenia PDFDocument11 pagesTrombocitopenia PDFbrigde_xNo ratings yet
- Konjungtivitis Gonore Pada BayiDocument16 pagesKonjungtivitis Gonore Pada Bayibrigde_xNo ratings yet
- Anti Platelet PreopDocument6 pagesAnti Platelet Preopbrigde_xNo ratings yet
- Heparin Infusion Guideline PDFDocument3 pagesHeparin Infusion Guideline PDFbrigde_xNo ratings yet
- The Changing Role of Beta-Blocker Therapy in Patients With CirrhosisDocument4 pagesThe Changing Role of Beta-Blocker Therapy in Patients With Cirrhosisbrigde_xNo ratings yet
- BMJ IrcDocument6 pagesBMJ IrcPaz RuizNo ratings yet
- 4 Possible Hemodynamic Profiles of HF: Congestion at RestDocument6 pages4 Possible Hemodynamic Profiles of HF: Congestion at Restbrigde_xNo ratings yet
- Abses HatiDocument6 pagesAbses HatiGilang Haliza100% (1)
- DPT and VaccineDocument13 pagesDPT and VaccineAlexisNo ratings yet
- Vacuna Hepatitis BDocument2 pagesVacuna Hepatitis Bluis alejandro rodriguez moraNo ratings yet
- Immunization ScheduleDocument2 pagesImmunization ScheduleTracy100% (1)
- Synflorix: Product MonographDocument40 pagesSynflorix: Product Monographabba,drNo ratings yet
- Barangay Monthly Inventory of Vaccinated PopulationDocument13 pagesBarangay Monthly Inventory of Vaccinated PopulationVince FulguerasNo ratings yet
- Monitoring Format HTH RI + MI - Apr2017Document3 pagesMonitoring Format HTH RI + MI - Apr2017Anonymous WgPzfGKR50% (2)
- Peace Corps MTG 300 ImmunizationDocument199 pagesPeace Corps MTG 300 ImmunizationAccessible Journal Media: Peace Corps DocumentsNo ratings yet
- Vaccinating GoatsDocument4 pagesVaccinating GoatsLisa VaughnNo ratings yet
- Cosili West Inventory of VaccinatedDocument28 pagesCosili West Inventory of VaccinatedLeigh BriosoNo ratings yet
- Pasien SafetyDocument37 pagesPasien SafetyDita Hafsari RitongaNo ratings yet
- 22-1 Plaintiff's Draft Amended Complaint Foley V BidenDocument66 pages22-1 Plaintiff's Draft Amended Complaint Foley V BidenDavid FoleyNo ratings yet
- CDC Booster RecommendationsDocument21 pagesCDC Booster RecommendationsNational Content DeskNo ratings yet
- BabyhoodDocument15 pagesBabyhoodJananee Rajagopalan100% (3)
- Handout - ADocument13 pagesHandout - AMadhu UpadhyayNo ratings yet
- DiphtheriaDocument10 pagesDiphtheriasenyorakathNo ratings yet
- Los Angeles Times - Vol. 140 No. 303 (02 Oct 2021)Document98 pagesLos Angeles Times - Vol. 140 No. 303 (02 Oct 2021)Xplosion01No ratings yet
- Infanrix Hexa SMPC 2016 08 16Document14 pagesInfanrix Hexa SMPC 2016 08 16walkrogNo ratings yet
- Hepatitis B Vaccine and Immunoglobulin Key ConceptDocument7 pagesHepatitis B Vaccine and Immunoglobulin Key ConceptMai Hoàng Dương QuangNo ratings yet
- Unknown PDFDocument56 pagesUnknown PDFMuhammad AdiNo ratings yet
- LPM: Extra-Parliamentary Questions - 25/03/2022 1Document20 pagesLPM: Extra-Parliamentary Questions - 25/03/2022 1Defimediagroup LdmgNo ratings yet
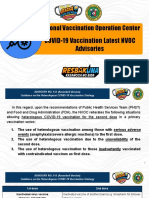
- Presentation On COVID 19 Latest AdvisoriesDocument35 pagesPresentation On COVID 19 Latest Advisoriesmondirah pandaNo ratings yet
- Confidential: Medical History and Personal Particulars of Students Joining at IIT MadrasDocument4 pagesConfidential: Medical History and Personal Particulars of Students Joining at IIT MadrasNehaNo ratings yet