You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Myofascial Pain Dysfunction Syndrome - A RevisitDocument9 pagesMyofascial Pain Dysfunction Syndrome - A RevisitRhea RejiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- EpilepsyDocument38 pagesEpilepsyJareena BegumNo ratings yet
- Che 225 Control of Communicable DiseasesDocument19 pagesChe 225 Control of Communicable DiseasesAbdullahi Bashir SalisuNo ratings yet
- Peter C. Gotzsche - Deadly Psychiatry and Organised Denial-ArtPeople (2015) PDFDocument335 pagesPeter C. Gotzsche - Deadly Psychiatry and Organised Denial-ArtPeople (2015) PDFicarosalerno75% (4)
- Guia NICE 2011 AutismoDocument51 pagesGuia NICE 2011 Autismomecho9002No ratings yet
- Wound CareDocument77 pagesWound CareNestor Balboa100% (1)
- Hydrolyzed CollagenDocument11 pagesHydrolyzed CollagenicarosalernoNo ratings yet
- Hydrolyzed CollagenDocument11 pagesHydrolyzed CollagenicarosalernoNo ratings yet
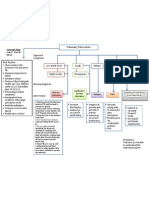
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Treatment Modalities Applicable To The Psychiatric ClientDocument53 pagesTreatment Modalities Applicable To The Psychiatric Clientnickybore100% (1)
- Efficacy of Corticosteroids in Non-Intensive Care Unit Patients With COVID-19 Pneumonia From The New York Metropolitan RegionDocument14 pagesEfficacy of Corticosteroids in Non-Intensive Care Unit Patients With COVID-19 Pneumonia From The New York Metropolitan RegionicarosalernoNo ratings yet
- 10 1016@j Eururo 2019 02 009Document9 pages10 1016@j Eururo 2019 02 009icarosalernoNo ratings yet
- 10.1001@jama.2018.6413 QSOFA Low Income CountriesDocument3 pages10.1001@jama.2018.6413 QSOFA Low Income CountriesicarosalernoNo ratings yet
- Practice Guidelines: Diagnosis of Stable Ischemic Heart Disease: Recommendations From The ACPDocument2 pagesPractice Guidelines: Diagnosis of Stable Ischemic Heart Disease: Recommendations From The ACPicarosalernoNo ratings yet
- AerosinusiteDocument4 pagesAerosinusiteicarosalernoNo ratings yet
- Chronic Benign Paroxysmal Positional Vertigo (BPPVDocument2 pagesChronic Benign Paroxysmal Positional Vertigo (BPPVicarosalernoNo ratings yet
- Fun With Modular ArithmeticDocument6 pagesFun With Modular ArithmeticicarosalernoNo ratings yet
- Family Laboratory For Medical Analysis: Test & SpecimenDocument1 pageFamily Laboratory For Medical Analysis: Test & SpecimenMohamad BadranNo ratings yet
- UntitledDocument17 pagesUntitledInggrid Aprilia ChristyNo ratings yet
- Gujarat Technological University: W.E.F. AY 2017-18Document3 pagesGujarat Technological University: W.E.F. AY 2017-18raj royelNo ratings yet
- Full Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadDocument11 pagesFull Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadFlip Body SpaNo ratings yet
- ApendikDocument4 pagesApendikSepti AyaNo ratings yet
- PediatricsDocument312 pagesPediatricsمحمد ابو مناضل الافينش100% (1)
- Detoxification:Management of AmaDocument3 pagesDetoxification:Management of AmaqueencelNo ratings yet
- Exercise #1 10Document10 pagesExercise #1 10John Paul FloresNo ratings yet
- Prevalence and Determinants of Substance Use Among Students at Kampala International University Western Campus, Ishaka Municipality Bushenyi District UgandaDocument18 pagesPrevalence and Determinants of Substance Use Among Students at Kampala International University Western Campus, Ishaka Municipality Bushenyi District UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- OlanzapineDocument1 pageOlanzapineKallie ChartrandNo ratings yet
- Endodontics Pain Control in Endodontics: Differential Diagnosis of Dental PainDocument4 pagesEndodontics Pain Control in Endodontics: Differential Diagnosis of Dental Painريام الموسويNo ratings yet
- 11 Human Body SystemDocument3 pages11 Human Body SystemCris EnriquezNo ratings yet
- ABC First Aid GuideDocument66 pagesABC First Aid GuideTze Ming VoonNo ratings yet
- Eye Lids and Lacrimal System: Dr. Binto Akturusiano, SPMDocument59 pagesEye Lids and Lacrimal System: Dr. Binto Akturusiano, SPMranz ibonkNo ratings yet
- Unit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheDocument5 pagesUnit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheioakasNo ratings yet
- Feeling GreatDocument243 pagesFeeling GreatSunny LamNo ratings yet
- Shellfish AllergyDocument23 pagesShellfish AllergyThessa Vee Capuno RioNo ratings yet
- TORCHDocument32 pagesTORCHJafar NoryNo ratings yet
- Exercise PrescriptionDocument53 pagesExercise PrescriptionEvangeline A. Alegre100% (1)
- Worksheet 4, Ubaidillah, 3BDocument6 pagesWorksheet 4, Ubaidillah, 3BUbay SegaNo ratings yet
- Needle Prick Injury & PreventionDocument17 pagesNeedle Prick Injury & Preventioniman zainuddinNo ratings yet
- Teaching Plan SampleDocument3 pagesTeaching Plan SampleSoleil MaxwellNo ratings yet
- Bilateral OsteoarthritisDocument58 pagesBilateral OsteoarthritisMaya VilNo ratings yet