You might also like
- Marketing Operations Term PaperDocument12 pagesMarketing Operations Term PaperShahzad AbbasNo ratings yet
- Pakistani English by Tariq Rehman PDFDocument101 pagesPakistani English by Tariq Rehman PDFHaroon Rasheed100% (1)
- Perceived Challenges of Using Web-Based Library Services by Students in Prof. Festus Aghabgo Nwako LibraryDocument6 pagesPerceived Challenges of Using Web-Based Library Services by Students in Prof. Festus Aghabgo Nwako LibraryShahzad AbbasNo ratings yet
- PDFDocument358 pagesPDFmsa_imegNo ratings yet
- PDFDocument358 pagesPDFmsa_imegNo ratings yet
- Advanced Dynamics GreenwoodDocument12 pagesAdvanced Dynamics GreenwoodShahzad AbbasNo ratings yet
- Medievalism and Orientalism Three Essays On Literature Architecture and Cultural Identity PDFDocument165 pagesMedievalism and Orientalism Three Essays On Literature Architecture and Cultural Identity PDFShahzad AbbasNo ratings yet
- Pakistan Digital Library Study PDFDocument7 pagesPakistan Digital Library Study PDFShahzad AbbasNo ratings yet
- The Renaissance. 6. The Formation of Classical MechanicsDocument15 pagesThe Renaissance. 6. The Formation of Classical MechanicsShahzad AbbasNo ratings yet
- The Renaissance. 6. The Formation of Classical MechanicsDocument15 pagesThe Renaissance. 6. The Formation of Classical MechanicsShahzad AbbasNo ratings yet
- Design and Construction of Oil Expeller Press With Structural Analysis of Screw With AnsysDocument6 pagesDesign and Construction of Oil Expeller Press With Structural Analysis of Screw With AnsysShahzad AbbasNo ratings yet
- PDFDocument358 pagesPDFmsa_imegNo ratings yet
- Institutional Repository Software DetailsDocument15 pagesInstitutional Repository Software DetailsShahzad AbbasNo ratings yet
- Marketing Strategies For Academic Libraries in The 21st CenturyDocument23 pagesMarketing Strategies For Academic Libraries in The 21st CenturyShahzad AbbasNo ratings yet
- Marketing Strategies For Digital Library Services1Document4 pagesMarketing Strategies For Digital Library Services1Shahzad AbbasNo ratings yet
- Un Pan 025134Document16 pagesUn Pan 025134Shahzad AbbasNo ratings yet
- Mario BottaDocument112 pagesMario BottaGabriel MazariegosNo ratings yet
- Factors Affecting Student Use of Web-Based ServicesDocument18 pagesFactors Affecting Student Use of Web-Based ServicesShahzad AbbasNo ratings yet
- National Librarian QualitiedDocument14 pagesNational Librarian QualitiedShahzad AbbasNo ratings yet
- Cloud Digital Repo Automation PresentationDocument14 pagesCloud Digital Repo Automation PresentationShahzad AbbasNo ratings yet
- Electromagnetic Field Theory: O HidéDocument203 pagesElectromagnetic Field Theory: O HidéAidaNo ratings yet
- Burnout: A Social Psychological AnalysisDocument12 pagesBurnout: A Social Psychological AnalysisShahzad AbbasNo ratings yet
- Electromagnetic Field Theory: O HidéDocument203 pagesElectromagnetic Field Theory: O HidéAidaNo ratings yet
- Information Literacy Tool For PromotionDocument8 pagesInformation Literacy Tool For PromotionShahzad AbbasNo ratings yet
- Electromagnetic Field Theory: O HidéDocument203 pagesElectromagnetic Field Theory: O HidéAidaNo ratings yet
- Repatriates and Reverse Knowledge Transfer in MNCsDocument20 pagesRepatriates and Reverse Knowledge Transfer in MNCsShahzad AbbasNo ratings yet
- Electromagnetic Field Theory: O HidéDocument203 pagesElectromagnetic Field Theory: O HidéAidaNo ratings yet
- wts2016 e PDFDocument165 pageswts2016 e PDFMikiKikiNo ratings yet
- Molecular Spectra and Molecular Structure - IV. Constants of Diatomic MoleculesDocument729 pagesMolecular Spectra and Molecular Structure - IV. Constants of Diatomic MoleculesShahzad Abbas100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
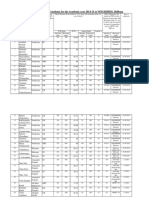
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Document10 pagesAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNo ratings yet
- Dmaema SDSDocument6 pagesDmaema SDSToffLinNo ratings yet
- Handbook of Laboratory Animal Science - Vol IIIDocument319 pagesHandbook of Laboratory Animal Science - Vol IIICarlos AlmeidaNo ratings yet
- FreezingDocument59 pagesFreezingManoj Rathod100% (1)
- Labcorp: Patient ReportDocument4 pagesLabcorp: Patient ReportAsad PrinceNo ratings yet
- Lasik VisionDocument3 pagesLasik VisionPrachurya SarmaNo ratings yet
- 11 - Chapter 7 PDFDocument41 pages11 - Chapter 7 PDFRakesh RakiNo ratings yet
- Biogas (Methane) EnglishDocument8 pagesBiogas (Methane) Englishveluthambi8888100% (1)
- 4bi1 - Jan22 2b QPDocument28 pages4bi1 - Jan22 2b QPXIN PEINo ratings yet
- As 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesDocument8 pagesAs 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesSAI Global - APACNo ratings yet
- Ageism PowerpointDocument11 pagesAgeism Powerpointapi-254132646No ratings yet
- 798 3072 1 PBDocument12 pages798 3072 1 PBMariana RitaNo ratings yet
- Method Development and Validation For Estimation of Moxifloxacin HCL in Tablet Dosage Form by RP HPLC Method 2153 2435.1000109Document2 pagesMethod Development and Validation For Estimation of Moxifloxacin HCL in Tablet Dosage Form by RP HPLC Method 2153 2435.1000109David SanabriaNo ratings yet
- Malaysia Deaths by Gender ReportDocument22 pagesMalaysia Deaths by Gender ReportNyazs IraNo ratings yet
- Barriers To Bystander CPR in Deprived Communities: Findings From A Qualitative StudyDocument11 pagesBarriers To Bystander CPR in Deprived Communities: Findings From A Qualitative Studygevowo3277No ratings yet
- Practitioner Review of Treatments for AutismDocument18 pagesPractitioner Review of Treatments for AutismAlexandra AddaNo ratings yet
- Legalizing abortion in the Philippines for women's health and rightsDocument2 pagesLegalizing abortion in the Philippines for women's health and rightsRosario Antoniete R. Cabilin100% (1)
- L-Sit ProgressionsDocument2 pagesL-Sit ProgressionsMattNo ratings yet
- HACCP Plan Distribution Cold ChainDocument23 pagesHACCP Plan Distribution Cold ChainHACCPEuropa86% (7)
- Name: Kashima Wright Candidate #: Centre #: Teacher: Ms. Morrison Territory: JamaicaDocument36 pagesName: Kashima Wright Candidate #: Centre #: Teacher: Ms. Morrison Territory: JamaicaKashima WrightNo ratings yet
- VITAMINS-Carol Jane Lorenzo, RMTDocument8 pagesVITAMINS-Carol Jane Lorenzo, RMTREYES, JAN MERCK M.No ratings yet
- MG English Consumer BookletDocument41 pagesMG English Consumer BookletAnh HoaiNo ratings yet
- Resolve Family Drainage CatetherDocument16 pagesResolve Family Drainage CatetherradeonunNo ratings yet
- Delivery Guide Flood PreparednessDocument23 pagesDelivery Guide Flood Preparednesshsehamad173No ratings yet
- UK Code of Practice For Tampon Manufactures and DistributorsDocument9 pagesUK Code of Practice For Tampon Manufactures and DistributorsFuzzy_Wood_PersonNo ratings yet
- MIDDLE ENGLISH TEST HEALTH VOCATIONAL HIGH SCHOOLDocument4 pagesMIDDLE ENGLISH TEST HEALTH VOCATIONAL HIGH SCHOOLZaenul WafaNo ratings yet
- Summer Internship Report on Chemist Behavior Towards Generic ProductsDocument30 pagesSummer Internship Report on Chemist Behavior Towards Generic ProductsBiswadeep PurkayasthaNo ratings yet
- Are You Dating Danger? An Interdisciplinary Approach To Evaluating The (In) Security of Android Dating Apps Author: Rushank ShettyDocument2 pagesAre You Dating Danger? An Interdisciplinary Approach To Evaluating The (In) Security of Android Dating Apps Author: Rushank ShettyAlexander RodriguezNo ratings yet
- Rosemont Hill Health CenterDocument14 pagesRosemont Hill Health CenterMona SahooNo ratings yet
- PE GCSE Revision Quiz - Updated With AnswersDocument40 pagesPE GCSE Revision Quiz - Updated With AnswersmohitNo ratings yet