You might also like
- Updated September 2016: PneumoniaDocument5 pagesUpdated September 2016: PneumoniaYidnekachew Girma Assefa100% (1)
- Pediatric History and Physical Exam GuideDocument7 pagesPediatric History and Physical Exam GuideIndunil AnuruddhikaNo ratings yet
- Essential Medicine ListDocument60 pagesEssential Medicine ListYidnekachew Girma AssefaNo ratings yet
- Pnemonia PDF 438.fullDocument21 pagesPnemonia PDF 438.fullYidnekachew Girma AssefaNo ratings yet
- Copy LN Pediatrics FinalDocument202 pagesCopy LN Pediatrics FinalYidnekachew Girma AssefaNo ratings yet
- Pediatrics History TakingDocument2 pagesPediatrics History TakingYidnekachew Girma AssefaNo ratings yet
- Our Drug Review Discusses The Diagnosis and Current Recommended Management Ofcommon URTIsDocument8 pagesOur Drug Review Discusses The Diagnosis and Current Recommended Management Ofcommon URTIsYidnekachew Girma AssefaNo ratings yet
- New MOC ResourcesDocument22 pagesNew MOC ResourcesYidnekachew Girma AssefaNo ratings yet
- PedaDocument2 pagesPedaYidnekachew Girma AssefaNo ratings yet
- Pneumonia Management in ChildrenDocument20 pagesPneumonia Management in ChildrenYidnekachew Girma AssefaNo ratings yet
- PedaDocument2 pagesPedaYidnekachew Girma AssefaNo ratings yet
- 10 Symptoms of PneumoniaDocument3 pages10 Symptoms of PneumoniaYidnekachew Girma AssefaNo ratings yet
- Consultation Eng History and PhysicalDocument28 pagesConsultation Eng History and PhysicalYidnekachew Girma AssefaNo ratings yet
- All Kids Get A Fever From Time To TimeDocument6 pagesAll Kids Get A Fever From Time To TimeYidnekachew Girma AssefaNo ratings yet
- 15Document4 pages15Yidnekachew Girma AssefaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sincope Vs Crisis - Lancet Neurol 2006 PDFDocument10 pagesSincope Vs Crisis - Lancet Neurol 2006 PDFLina HerreraNo ratings yet
- TBCP GuideDocument20 pagesTBCP GuideJustin CreekNo ratings yet
- Sigmoid Volvulus: Vertical Incision) (Suspected To Be Acute and Not ChronicDocument3 pagesSigmoid Volvulus: Vertical Incision) (Suspected To Be Acute and Not ChronicTan Hing LeeNo ratings yet
- PL JanDocument83 pagesPL JanMYD98Official MYDNo ratings yet
- Oxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDocument21 pagesOxfordshire ADULT Antimicrobial Prescribing Guidelines For Primary CareDan IonescuNo ratings yet
- RSIA Rizki Bunda Slow Moving Drug ListDocument4 pagesRSIA Rizki Bunda Slow Moving Drug Listzolla verbiantiNo ratings yet
- Metformin in PCOSDocument5 pagesMetformin in PCOSbalaramNo ratings yet
- List of Basic Essential Medicines Ministry of Health Seychelles 2010Document14 pagesList of Basic Essential Medicines Ministry of Health Seychelles 2010portosinNo ratings yet
- Case StudyDocument13 pagesCase StudyLeong Ka YeeNo ratings yet
- Drug Study..Document4 pagesDrug Study..Micah SalesNo ratings yet
- Drug StudyDocument6 pagesDrug StudySoleil MaxwellNo ratings yet
- What Is Acute BronchitisDocument11 pagesWhat Is Acute BronchitisKerri-DojhnHallNo ratings yet
- Super Salida Especial-Mes de Junio ActualizadaDocument90 pagesSuper Salida Especial-Mes de Junio ActualizadaDiego PazmiñoNo ratings yet
- Family Medicine Shelf Review - PPTX (Read-Only)Document142 pagesFamily Medicine Shelf Review - PPTX (Read-Only)Alejandro Bocanegra Osuna58% (19)
- GENERICSKING TRADING INC PRICE LISTDocument10 pagesGENERICSKING TRADING INC PRICE LISTCrystal NgNo ratings yet
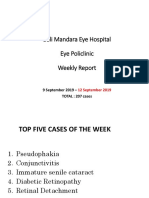
- Bali Mandara Eye Hospital Eye Policlinic Weekly Report: 9 September 2019 - TOTAL: 207 CasesDocument23 pagesBali Mandara Eye Hospital Eye Policlinic Weekly Report: 9 September 2019 - TOTAL: 207 CasesLipo DuoNo ratings yet
- Dosage and effects of ampicillinDocument1 pageDosage and effects of ampicillinkimglaidyl bontuyanNo ratings yet
- Dipenhydramine Drug-StudyDocument1 pageDipenhydramine Drug-StudyTrisha CayabyabNo ratings yet
- Data Publikasi Jurnal Internasional Dan Nasional Serta Haki Dosen Departemen Keperawatan Maternitas Fakultas Keperawatan Unpad Tahun 2019Document2 pagesData Publikasi Jurnal Internasional Dan Nasional Serta Haki Dosen Departemen Keperawatan Maternitas Fakultas Keperawatan Unpad Tahun 2019Enta fitriyaNo ratings yet
- Hypertension Management-1Document15 pagesHypertension Management-1Ali Sibra MulluziNo ratings yet
- Azithromycin WarningsDocument4 pagesAzithromycin WarningsChristian Angelo LeonorNo ratings yet
- Whooping Cough Pertussis PDFDocument2 pagesWhooping Cough Pertussis PDFFikri RamadhanNo ratings yet
- ORE DrugsDocument4 pagesORE DrugsKhalid G. AzouniNo ratings yet
- Morning Report September, 10 2015: Supervisor: Dr. Agus Thoriq, Spog DM Jaga: RianDocument15 pagesMorning Report September, 10 2015: Supervisor: Dr. Agus Thoriq, Spog DM Jaga: RianRian Segal HidajatNo ratings yet
- Reckeweg MedicinesDocument83 pagesReckeweg MedicinesRAGHVENDRA100% (2)
- MF Mmi PDFDocument4 pagesMF Mmi PDFAbou Tebba SamNo ratings yet
- Pulmonary TuberculosisDocument17 pagesPulmonary TuberculosisRobert Dominic GonzalesNo ratings yet
- Cefuroxime Nursing Responsibilities for Indications, Mechanism of Action, Side Effects and ContraindicationsDocument2 pagesCefuroxime Nursing Responsibilities for Indications, Mechanism of Action, Side Effects and ContraindicationsKate TergaNo ratings yet
- Hubungan Pengetahuan, Sikap dan Tindakan Keluarga dengan Pencegahan TB Paru AktifDocument124 pagesHubungan Pengetahuan, Sikap dan Tindakan Keluarga dengan Pencegahan TB Paru AktifWilma arifinNo ratings yet
- CH 57 Care of Patients With Inflammatory Intestinal DisordersDocument19 pagesCH 57 Care of Patients With Inflammatory Intestinal Disordersjrflores1284No ratings yet