You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Answer Key - Epi Midterm Study Guide - 2018Document8 pagesAnswer Key - Epi Midterm Study Guide - 2018Sanaz NiksefatNo ratings yet
- Gujarat ReportDocument34 pagesGujarat ReportashishldrpNo ratings yet
- Marshall Community Letter: Person at Middle School Tests Positive For CoronavirusDocument1 pageMarshall Community Letter: Person at Middle School Tests Positive For CoronavirusJoy M. HosfordNo ratings yet
- Epidemiology MCH 101Document96 pagesEpidemiology MCH 101Christiaan Gaye B. PilayNo ratings yet
- Maternal and Child Health ProblemDocument5 pagesMaternal and Child Health Problemvikas takNo ratings yet
- MedicinesDocument9 pagesMedicinesAshishGroverNo ratings yet
- Epidemiology PPT NewDocument100 pagesEpidemiology PPT NewSujatha Aluguri100% (2)
- Sas 15Document5 pagesSas 15Kristinelou Marie ReynaNo ratings yet
- Knowledge, Attitude and Practices of Rural Mothers With Children Under Five Years of Age About Vaccination A Non Experimental StudyDocument9 pagesKnowledge, Attitude and Practices of Rural Mothers With Children Under Five Years of Age About Vaccination A Non Experimental StudyUlil Amri PramadaniNo ratings yet
- Rekapan Jan JuliDocument36 pagesRekapan Jan JuligendhisNo ratings yet
- Tutorial Epid TUTORDocument7 pagesTutorial Epid TUTORStefanus Tabbo0% (1)
- Global Cholera Epidemiology: Opportunities To Reduce The Burden of Cholera by 2030Document4 pagesGlobal Cholera Epidemiology: Opportunities To Reduce The Burden of Cholera by 2030Gufron MustofaNo ratings yet
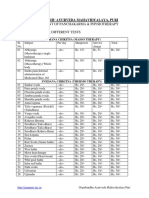
- Rate Chart PanchakarmaDocument2 pagesRate Chart PanchakarmayogasanaNo ratings yet
- Audit - Infection Control - 20180607 - 1557 PDFDocument3 pagesAudit - Infection Control - 20180607 - 1557 PDFJailie L. EnguioNo ratings yet
- WHO-Preconception Care To Reduce Maternal and Childhood Mortality and MorbidityDocument77 pagesWHO-Preconception Care To Reduce Maternal and Childhood Mortality and MorbidityAditya TejabaswaraNo ratings yet
- Vaccination CertificateDocument1 pageVaccination CertificateSivaa BapanapalliNo ratings yet
- 5 - Revised - Self-Assessment Tool For Selected MNCHN Indicators - August14,2014Document92 pages5 - Revised - Self-Assessment Tool For Selected MNCHN Indicators - August14,2014Glenn L. RavanillaNo ratings yet
- Manuskrip NewDocument4 pagesManuskrip NewbaesootzuNo ratings yet
- KAP Questionnaire For Health WorkersDocument3 pagesKAP Questionnaire For Health WorkersDharma Reddy PashapuNo ratings yet
- This Study Resource WasDocument2 pagesThis Study Resource Waswriter topNo ratings yet
- Biostatistics - EpidemiologyDocument506 pagesBiostatistics - Epidemiologyprakash poudelNo ratings yet
- DM No. 272, S. 2022 - Conduct of Community or School Based Immunization On Measles Rubella Vaccine From October To December 2022Document5 pagesDM No. 272, S. 2022 - Conduct of Community or School Based Immunization On Measles Rubella Vaccine From October To December 2022Alexander CruzNo ratings yet
- Persuasive (SAMPLE) Speech OutlineDocument3 pagesPersuasive (SAMPLE) Speech OutlineJosephine NavarroNo ratings yet
- Syllabus-VPE-321 Veterinary Epidemiology and ZoonosesDocument1 pageSyllabus-VPE-321 Veterinary Epidemiology and ZoonosesRamesh BeniwalNo ratings yet
- Gec eDocument1 pageGec eMaria Venus MontoloNo ratings yet
- Wang Yunshan ReflectionDocument4 pagesWang Yunshan Reflectionapi-286742915100% (1)
- 3.2 Risk Rate Measures Cohort Studies PDFDocument3 pages3.2 Risk Rate Measures Cohort Studies PDFSherida GibbsNo ratings yet
- Journal ReadingDocument13 pagesJournal ReadingFahrika Luthfi AfiqohNo ratings yet
- Basic Nip Chapter 1 Intro To NipDocument15 pagesBasic Nip Chapter 1 Intro To NipLower Balulang Health CenterNo ratings yet
- TobaccoDocument4 pagesTobaccoapi-341002616100% (1)