You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
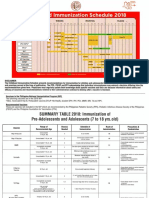
- Pedia ImmunizationDocument4 pagesPedia ImmunizationTeves AdrianNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Gout CPG Manuscript - PJIM 072808Document16 pagesGout CPG Manuscript - PJIM 072808Francis CastellNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Endocrinopathies Are Now Well Recognized. These Include Myopathies Associated With ThyroidDocument10 pagesEndocrinopathies Are Now Well Recognized. These Include Myopathies Associated With ThyroidTeves AdrianNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Cardiac Rehab: ND RD TH NDDocument3 pagesCardiac Rehab: ND RD TH NDDoodsDiagoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- TheraEx PVD OrgDocument1 pageTheraEx PVD OrgTeves AdrianNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- TheraEx PVD OrgDocument1 pageTheraEx PVD OrgTeves AdrianNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- TheraEx PVDDocument8 pagesTheraEx PVDDoodsDiagoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Cranial NervesDocument7 pagesCranial NervesTeves AdrianNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Harrison's CoughDocument1 pageHarrison's CoughTeves AdrianNo ratings yet
- 400-750 NM AccommodationDocument2 pages400-750 NM AccommodationTeves AdrianNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Scoliosis TreatmentDocument3 pagesScoliosis TreatmentTeves AdrianNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Prognostic Factors and Management of Patients With Choanal AtresiaDocument7 pagesPrognostic Factors and Management of Patients With Choanal Atresiafarah maulida martaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Cobalamin in Companion AnimalsDocument8 pagesCobalamin in Companion AnimalsFlávia UchôaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Salient Features of The National Health Policy - 2017: July 2019Document3 pagesSalient Features of The National Health Policy - 2017: July 2019Deepanshu JharkhandeNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- b1 ChecklistDocument2 pagesb1 ChecklistRoryNo ratings yet
- Chemistry Investigatory Project 2017-18Document29 pagesChemistry Investigatory Project 2017-18Ashok KumarNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Role of N-Acetylcysteine in The Health and Production of Poultry.Document9 pagesRole of N-Acetylcysteine in The Health and Production of Poultry.Abdullah Saleem100% (1)
- Course Task 19Document1 pageCourse Task 19Laira CañeteNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Chordoma Current Concepts Management and Future DirectionsDocument8 pagesChordoma Current Concepts Management and Future DirectionsChristian AdeNo ratings yet
- Protozoa and Fungi Culturing in The LabDocument7 pagesProtozoa and Fungi Culturing in The LabrorenNo ratings yet
- How To Help Poor Countries: Nancy Birdsall, Dani Rodrik, and Arvind SubramanianDocument17 pagesHow To Help Poor Countries: Nancy Birdsall, Dani Rodrik, and Arvind SubramanianMarcus MonocayNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Test Planner-2022-2023 (CF+OYM) Phase-02 - FT, & TE Version 1.0-1Document4 pagesTest Planner-2022-2023 (CF+OYM) Phase-02 - FT, & TE Version 1.0-1Dev SoniNo ratings yet
- Effect of Dragon Fruit On Lipid ProfileDocument2 pagesEffect of Dragon Fruit On Lipid ProfileElindah Ayunin ArrumNo ratings yet
- Wolf PresentationDocument35 pagesWolf PresentationTahir Bin AbdullahNo ratings yet
- CATARACTDocument82 pagesCATARACTRavi KushwahaNo ratings yet
- Arthritis E-Book DF PDFDocument14 pagesArthritis E-Book DF PDFManuel Anthony Lopez0% (1)
- Molecular Biology R - F - Weaver 5th EdDocument1 pageMolecular Biology R - F - Weaver 5th EdAlapan NandaNo ratings yet
- Target Product Profile Imbruvica - IbrutinibDocument1 pageTarget Product Profile Imbruvica - IbrutinibDiti ShahNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- RRL LocalinternationalDocument11 pagesRRL LocalinternationalkdfhjfhfNo ratings yet
- A Review Paper On Scope of Big Data Analysis in Heath INFORMATICSDocument8 pagesA Review Paper On Scope of Big Data Analysis in Heath INFORMATICSMohamed Aly SowNo ratings yet
- This Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCDocument9 pagesThis Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCsinnanancyNo ratings yet
- Wing 1981 AspergerDocument15 pagesWing 1981 Asperger__aguNo ratings yet
- The Socket Shield Technique Case ReportDocument5 pagesThe Socket Shield Technique Case ReportAhmed Mohammed Saaduddin SapriNo ratings yet
- TOI AhmadabadDocument24 pagesTOI AhmadabadJugarNo ratings yet
- Intensive Care For ChildrenDocument98 pagesIntensive Care For ChildrenTufail MemonNo ratings yet
- Daycare Fact SheetDocument1 pageDaycare Fact SheetJoana R. SilvaNo ratings yet
- Pakpak LawinDocument16 pagesPakpak Lawinmaylene estoque0% (1)
- Kidney DiseasesDocument22 pagesKidney Diseasesphoto copyhemnNo ratings yet
- Giant Cell TumourDocument61 pagesGiant Cell Tumourvictormoirangthem100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Export Act 1963Document27 pagesExport Act 1963Anonymous OPix6Tyk5INo ratings yet
- Breastfeeding QuestionnaireDocument2 pagesBreastfeeding QuestionnaireDr Puteri Nur Sabrina Binti Mohd HanapiNo ratings yet