You might also like
- Urethral DischargeDocument26 pagesUrethral DischargeZahra ArainNo ratings yet
- Urethritis: Continuing Education ActivityDocument8 pagesUrethritis: Continuing Education ActivityMutiara AmaliaNo ratings yet
- UrethritisDocument11 pagesUrethritisgreggy_rebel17No ratings yet
- Includes: Urinary Tract Infections Genital Tract Infections Viral Sexually Transmitted Diseases Bacterial Sexual Transmitted DiseasesDocument37 pagesIncludes: Urinary Tract Infections Genital Tract Infections Viral Sexually Transmitted Diseases Bacterial Sexual Transmitted DiseasesDon Pelicio NgohoNo ratings yet
- Infectious Causes of Dysuria in Adult MenDocument5 pagesInfectious Causes of Dysuria in Adult MenFrancisco Javier Contreras MoralesNo ratings yet
- Gonorrhea - Practice Essentials, Background, Pathophysiology Sumber 13Document15 pagesGonorrhea - Practice Essentials, Background, Pathophysiology Sumber 13Anizha AdriyaniNo ratings yet
- By: Jennifer Vu, Teresa Kodi, Emily Dang, James Baawuo and Yesenia AlmanzaDocument19 pagesBy: Jennifer Vu, Teresa Kodi, Emily Dang, James Baawuo and Yesenia AlmanzajbaawuoNo ratings yet
- Sexually Transmitted DiseasesDocument71 pagesSexually Transmitted DiseasesAkwu AkwuNo ratings yet
- Urinary System and Its PathologiesDocument23 pagesUrinary System and Its Pathologiesngachangong victorineNo ratings yet
- Sexually Transmitted InfectionsDocument48 pagesSexually Transmitted InfectionsYsabella LlanetaNo ratings yet
- UrethritisDocument11 pagesUrethritismarej143No ratings yet
- Sexually Transmitted Infections (Sti) Ii: Return To SyllabusDocument15 pagesSexually Transmitted Infections (Sti) Ii: Return To SyllabusANGGITA LARASATI PURBANINGRUMNo ratings yet
- Genitourinary SystemDocument7 pagesGenitourinary SystemMary Angel VelascoNo ratings yet
- GonorrheaDocument53 pagesGonorrheaapi-1991639975% (4)
- Sexually Transmitted Infections - Hatem Sadek PresentationDocument36 pagesSexually Transmitted Infections - Hatem Sadek PresentationHatem SadekNo ratings yet
- Sti 2018 LseDocument67 pagesSti 2018 LsespinosumNo ratings yet
- Urinary Tract Infections DR Moses KazevuDocument23 pagesUrinary Tract Infections DR Moses KazevuMoses Jr KazevuNo ratings yet
- Epididymitis and OrchitisDocument11 pagesEpididymitis and Orchitiscitra08No ratings yet
- URETHRITIS - Yulia W 026Document20 pagesURETHRITIS - Yulia W 026Yulia WidiastutiNo ratings yet
- Tubo Ovarian Abcess (Abses Tuba-Ovari)Document4 pagesTubo Ovarian Abcess (Abses Tuba-Ovari)Muhammad Naqiuddin JalaluddinNo ratings yet
- Wikipedia - Epididymitis (CHECKED)Document6 pagesWikipedia - Epididymitis (CHECKED)pixoguiasNo ratings yet
- OrchitisDocument5 pagesOrchitisNader SmadiNo ratings yet
- TrichomoniasisDocument23 pagesTrichomoniasisSaba Siva50% (2)
- Sexually Transmitted Infections GuideDocument89 pagesSexually Transmitted Infections GuidegibreilNo ratings yet
- Sindrome Duh Genital GODocument9 pagesSindrome Duh Genital GOIntan PermataNo ratings yet
- STI Clinical GuideDocument83 pagesSTI Clinical Guidebekbekk cabahugNo ratings yet
- 7 PyuriaDocument19 pages7 PyuriaFarihatun NisaNo ratings yet
- Urinary Tract InfectionDocument46 pagesUrinary Tract Infectionbest batiNo ratings yet
- Reproductive Tract InformationDocument14 pagesReproductive Tract InformationGonçalo BaptistaNo ratings yet
- Urinary Tract Infection: By: Yoavita Moderator: Dr. Ati Rastini Ri, SPPK (K)Document40 pagesUrinary Tract Infection: By: Yoavita Moderator: Dr. Ati Rastini Ri, SPPK (K)ChristinaNo ratings yet
- Sexually Transmitted InfectionsDocument10 pagesSexually Transmitted InfectionsStar CruiseNo ratings yet
- Acute CervicitisDocument9 pagesAcute CervicitisVicobeingoNo ratings yet
- Causes and management of common vaginal dischargesDocument8 pagesCauses and management of common vaginal dischargesMELVYN HAROLD CHAVEZ MAURICIONo ratings yet
- Chapter 53: Nursing Management: Sexually Transmitted DiseasesDocument4 pagesChapter 53: Nursing Management: Sexually Transmitted DiseasesjefrocNo ratings yet
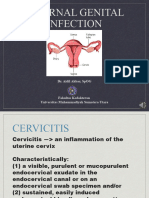
- Daring Aidil Akbar Internal Genital InfectionDocument29 pagesDaring Aidil Akbar Internal Genital InfectionrakaNo ratings yet
- Genitourinary Chlamydial Infection GuideDocument18 pagesGenitourinary Chlamydial Infection GuideNatalie AlcântaraNo ratings yet
- Pelvic Inflammatory DiseaseDocument15 pagesPelvic Inflammatory Diseaseashleenriya832No ratings yet
- Trusted Medical Answers-In Seconds.: GonorrheaDocument7 pagesTrusted Medical Answers-In Seconds.: GonorrheantnquynhproNo ratings yet
- By: Shazleen Farhana Anggun Lestary Advisor: Dr. Diana Muchsin Supervisor: Dr. Asnawi Madjid, SP - KK, MARSDocument25 pagesBy: Shazleen Farhana Anggun Lestary Advisor: Dr. Diana Muchsin Supervisor: Dr. Asnawi Madjid, SP - KK, MARSShazleen FarhanaNo ratings yet
- STD 1Document56 pagesSTD 1PrakritiNo ratings yet
- Non Gonococcal UrethritisDocument4 pagesNon Gonococcal UrethritisEunice TrongcoNo ratings yet
- Homeopathic Treatment of Urethritis Thomas A. Kruzel, N. DDocument6 pagesHomeopathic Treatment of Urethritis Thomas A. Kruzel, N. DAtmayadi GunawanNo ratings yet
- RPS Penyakit KelaminDocument133 pagesRPS Penyakit KelaminArdana WindriyaNo ratings yet
- Urethral Discharge in Male, 1987Document6 pagesUrethral Discharge in Male, 1987ElisabethJaniceRusliNo ratings yet
- Female Genital Inflammatory DiseasesDocument39 pagesFemale Genital Inflammatory DiseaseseveeNo ratings yet
- GonorrheaDocument3 pagesGonorrheaRe-ann Mae F. MendozaNo ratings yet
- Evaluation of Dysuria in AdultsDocument8 pagesEvaluation of Dysuria in AdultspapermintNo ratings yet
- The Pathophysiology of Urinary Tract Infections: Practical Interpretations of Commonly Used TermsDocument6 pagesThe Pathophysiology of Urinary Tract Infections: Practical Interpretations of Commonly Used TermsPaullette SanjuanNo ratings yet
- Tai Lieu Tieng Anh Cho Sinh Vien Bai Nhiem Khuan Duong Tiet NieuDocument3 pagesTai Lieu Tieng Anh Cho Sinh Vien Bai Nhiem Khuan Duong Tiet NieuLê Mỹ Khánh LyNo ratings yet
- Orchits ManagementDocument9 pagesOrchits ManagementMarshall ThompsonNo ratings yet
- Trichomoniasis: Causes, Symptoms and Treatment of Trichomonas vaginalis InfectionDocument17 pagesTrichomoniasis: Causes, Symptoms and Treatment of Trichomonas vaginalis InfectionAndi MuhammadNo ratings yet
- Upper Genital Tract Infection (PID)Document24 pagesUpper Genital Tract Infection (PID)Tofitofi TofiNo ratings yet
- MICROBIOLOGY OF GENITOURINARY TRACT-2 (Julia Hartati, DR.)Document24 pagesMICROBIOLOGY OF GENITOURINARY TRACT-2 (Julia Hartati, DR.)Ayi Abdul BasithNo ratings yet
- Gonorrhea: Neisseria GonorrhoeaeDocument60 pagesGonorrhea: Neisseria GonorrhoeaeRikki OkNo ratings yet
- Review of Aetiology and Management of Testicular Abscess and Case Reports On Testicle Sparing Management of Testicular AbscessDocument5 pagesReview of Aetiology and Management of Testicular Abscess and Case Reports On Testicle Sparing Management of Testicular AbscessBodat BodatsNo ratings yet
- 2028-Article Text-6551-1-10-20230128Document5 pages2028-Article Text-6551-1-10-20230128hellowqueenyNo ratings yet
- Urinary Tract InfectionDocument50 pagesUrinary Tract Infectionpokhara gharipatanNo ratings yet
- Medical Microbiology: Sti (STD)Document90 pagesMedical Microbiology: Sti (STD)Brother GeorgeNo ratings yet
- Reproductive System DiseasesDocument5 pagesReproductive System DiseasesMichael Vincent P.No ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Pead 1 - NeonatologyDocument21 pagesPead 1 - NeonatologybbyesNo ratings yet
- Advanced Life Support AssessmentDocument1 pageAdvanced Life Support AssessmentbbyesNo ratings yet
- SSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExamDocument4 pagesSSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExambbyesNo ratings yet
- Tocolytics in PretermDocument13 pagesTocolytics in PretermbbyesNo ratings yet
- HMO Surgical PositionDocument4 pagesHMO Surgical PositionbbyesNo ratings yet
- Prenatal ScreeningDocument26 pagesPrenatal ScreeningbbyesNo ratings yet
- Early Pregnancy ComplciationsDocument43 pagesEarly Pregnancy ComplciationsbbyesNo ratings yet
- Substance Abuse in PregnancyDocument151 pagesSubstance Abuse in PregnancybbyesNo ratings yet
- Guideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisDocument18 pagesGuideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisbbyesNo ratings yet
- Position Description ENTDocument3 pagesPosition Description ENTbbyesNo ratings yet
- BASIC Course Gosford June 2021Document3 pagesBASIC Course Gosford June 2021bbyesNo ratings yet
- Training Manual 2020Document53 pagesTraining Manual 2020bbyesNo ratings yet
- Surgical - Information GuideDocument2 pagesSurgical - Information GuidebbyesNo ratings yet
- C SpineDocument44 pagesC SpinebbyesNo ratings yet
- Organisation Chart - TraineeDocument1 pageOrganisation Chart - TraineebbyesNo ratings yet
- Right VATS Pleural BiopsyDocument4 pagesRight VATS Pleural BiopsybbyesNo ratings yet
- Ischkwa DiagramDocument1 pageIschkwa DiagrambbyesNo ratings yet
- Atrial Fibrillation Managing Acute Atrial FibrillationDocument8 pagesAtrial Fibrillation Managing Acute Atrial FibrillationbbyesNo ratings yet
- Upper GI BleedDocument8 pagesUpper GI BleedbbyesNo ratings yet
- Varicose VeinDocument6 pagesVaricose VeinbbyesNo ratings yet
- RHDDocument130 pagesRHDDeepu RajendranNo ratings yet
- ECGs - UpdatedDocument26 pagesECGs - UpdatedbbyesNo ratings yet
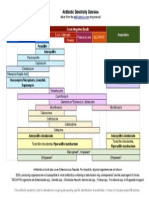
- Antibiotic Sensitivity Overview for Gram Positive Cocci, Gram Negative Bacilli and AnaerobesDocument1 pageAntibiotic Sensitivity Overview for Gram Positive Cocci, Gram Negative Bacilli and AnaerobesGuillermo Damian RodriguezNo ratings yet
- Infections in PregnancyDocument11 pagesInfections in PregnancybbyesNo ratings yet
- Prof PracDocument3 pagesProf PracbbyesNo ratings yet
- Shoulder PainDocument5 pagesShoulder PainbbyesNo ratings yet
- Pump Manual TextDocument17 pagesPump Manual TextbbyesNo ratings yet
- Weekly SDS Topics: Week 3Document1 pageWeekly SDS Topics: Week 3bbyesNo ratings yet
- Curriculum Vitae: Shaikh Rukshana SalimDocument2 pagesCurriculum Vitae: Shaikh Rukshana SalimMithlesh SinghNo ratings yet
- CandidiasisDocument27 pagesCandidiasisWr Newgate50% (2)
- CCG Elderholme Responses To Final ReportDocument24 pagesCCG Elderholme Responses To Final ReportLeonard BeddowsNo ratings yet
- Shallo El Hard I90 BDocument2 pagesShallo El Hard I90 Belhard shalloNo ratings yet
- Course Task Unit 3Document2 pagesCourse Task Unit 3BSN 1-YA-22 ELITIONG, MARY JEAN A.No ratings yet
- The Health Bank (THB) Connected Care Program A Pilot Study of Remote Monitoring For The Management of Chronic Conditions Focusing On DiabetesDocument5 pagesThe Health Bank (THB) Connected Care Program A Pilot Study of Remote Monitoring For The Management of Chronic Conditions Focusing On DiabetesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Role of Ayurveda in Treating Cervical ErosionDocument9 pagesRole of Ayurveda in Treating Cervical Erosionrazvan rotaruNo ratings yet
- Evidence 1.15.9-Change Log To Demonstrate The Differences Between 2017 and 2021 Edition PDFDocument13 pagesEvidence 1.15.9-Change Log To Demonstrate The Differences Between 2017 and 2021 Edition PDFKhalid ElwakilNo ratings yet
- Hypertension: Facts, Causes, Prevention and TreatmentDocument18 pagesHypertension: Facts, Causes, Prevention and TreatmentasepNo ratings yet
- Pulsed Dye Laser Therapy For Cutaneous Vascular LesionsDocument3 pagesPulsed Dye Laser Therapy For Cutaneous Vascular LesionsOogway MasterNo ratings yet
- Helping Babies Breathe™ 06.27.2014Document18 pagesHelping Babies Breathe™ 06.27.2014Emily EresumaNo ratings yet
- Additional File 3 - JBI ChecklistsDocument10 pagesAdditional File 3 - JBI Checklistsbella friscaamaliaNo ratings yet
- EthambutolDocument1 pageEthambutolSibel ErtuğrulNo ratings yet
- Pediatric Ophthalmology DR - JusufDocument25 pagesPediatric Ophthalmology DR - JusufAmira AlhaddarNo ratings yet
- Critical Reasoning Questions for Schizoaffective DisorderDocument2 pagesCritical Reasoning Questions for Schizoaffective DisorderjessyNo ratings yet
- NCP DrainageDocument3 pagesNCP DrainageRuby GuarinNo ratings yet
- Den 437Document6 pagesDen 437Prince AhmedNo ratings yet
- BBBFDocument3 pagesBBBFSkAliHassanNo ratings yet
- Student Response Sheet: PurposeDocument4 pagesStudent Response Sheet: PurposeYoshi NNo ratings yet
- MalariaDocument38 pagesMalariaMehroze FatimaNo ratings yet
- Pathology Situational EthicsDocument28 pagesPathology Situational Ethicsmohitsingla_86No ratings yet
- Guidelines For 1st Quarter AY 2022-2023Document12 pagesGuidelines For 1st Quarter AY 2022-2023Zhen ChiNo ratings yet
- Healthcare Stats - Assignment #2Document6 pagesHealthcare Stats - Assignment #2erickgregs0% (1)
- Hepatic Dysfunction in Dengue Fever - A ProspectiveDocument20 pagesHepatic Dysfunction in Dengue Fever - A ProspectiveSanjay RaoNo ratings yet
- Epidemiology & Health Information: NU1103 Tara Brookes @tarapb8Document40 pagesEpidemiology & Health Information: NU1103 Tara Brookes @tarapb8smartisaacNo ratings yet
- Endometritis Unrelated To Pregnancy - UpToDateDocument9 pagesEndometritis Unrelated To Pregnancy - UpToDateLeoberto Batista Pereira SobrinhoNo ratings yet
- Helicopter interventions for polytraumatized patients in North-East RomaniaDocument2 pagesHelicopter interventions for polytraumatized patients in North-East RomaniaN.DanielaNo ratings yet
- How To Setup Biotrans ?Document21 pagesHow To Setup Biotrans ?Agoes TreeyantNo ratings yet
- Medication Safety UnitDocument58 pagesMedication Safety Unitfarmasi_hmNo ratings yet
- NEET MDS 2021 Recall 151-200 Questions PDFDocument183 pagesNEET MDS 2021 Recall 151-200 Questions PDFMahima Mishra100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)