You might also like
- SITXFIN003 Class ActivityDocument6 pagesSITXFIN003 Class Activitymachuky jrNo ratings yet
- SITXFIN004 Prepare and Monitor BudgetsNOTE1Document34 pagesSITXFIN004 Prepare and Monitor BudgetsNOTE1machuky jrNo ratings yet
- Assessment Manage FinanceDocument34 pagesAssessment Manage Financemachuky jrNo ratings yet
- BSBTEC601 Task 1Document3 pagesBSBTEC601 Task 1machuky jrNo ratings yet
- Business Model - Lean Canvas: by Ash MauryaDocument16 pagesBusiness Model - Lean Canvas: by Ash Mauryamachuky jrNo ratings yet
- Chandragupta & AshokaDocument42 pagesChandragupta & Ashokamachuky jrNo ratings yet
- Value Proposition Canvas: Gain Creators GainsDocument1 pageValue Proposition Canvas: Gain Creators Gainsmachuky jrNo ratings yet
- The Star 13th FebDocument48 pagesThe Star 13th Febmachuky jrNo ratings yet
- Problem Solution Unique Value Proposition Unfair Advantage Customer SegmentsDocument2 pagesProblem Solution Unique Value Proposition Unfair Advantage Customer Segmentsmachuky jrNo ratings yet
- Problem Solution Unique Value Proposition Unfair Advantage Customer SegmentsDocument2 pagesProblem Solution Unique Value Proposition Unfair Advantage Customer Segmentsmachuky jrNo ratings yet
- Disclosure Strategies For Pollution Control: Environmental and Resource Economics 11 (3-4) : 587-602, 1998Document16 pagesDisclosure Strategies For Pollution Control: Environmental and Resource Economics 11 (3-4) : 587-602, 1998machuky jrNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayNo ratings yet
- ABC Imaging 1 - The SpineDocument145 pagesABC Imaging 1 - The SpineAna-Maria PaunescuNo ratings yet
- Drug Study I MetronidazoleDocument2 pagesDrug Study I MetronidazoleKimberly Ann Aquino50% (2)
- Combank NotesDocument7 pagesCombank NotesVee MendNo ratings yet
- Fundamental Rationale and AnswersDocument237 pagesFundamental Rationale and AnswersNorminaKiramAkmadNo ratings yet
- NURS 4045 Adult Health Competencies II Texas Woman's University Patient Data SheetDocument11 pagesNURS 4045 Adult Health Competencies II Texas Woman's University Patient Data Sheetuyen doNo ratings yet
- Neuroimaging Self Assessment Colour ReviewDocument228 pagesNeuroimaging Self Assessment Colour ReviewHamza Arjah100% (1)
- Di, Siadh, CSW Tabel PerbedaanDocument17 pagesDi, Siadh, CSW Tabel PerbedaanMichael Tambunan100% (1)
- Ophthalmology - Diseases of The EyelidsDocument9 pagesOphthalmology - Diseases of The EyelidsjbtcmdtjjvNo ratings yet
- MAKING SENSE OF PSYCHIATRY: Our Impenetrable Personal ComputerDocument16 pagesMAKING SENSE OF PSYCHIATRY: Our Impenetrable Personal ComputerPaul Minot MDNo ratings yet
- Common Prescribed DrugsDocument33 pagesCommon Prescribed DrugsGlessica You50% (4)
- Similarities and Differences VocabularyDocument9 pagesSimilarities and Differences VocabularyAliNo ratings yet
- Test Bank For Goulds Pathophysiology For The Health Professions 5th Edition by VanmeterDocument7 pagesTest Bank For Goulds Pathophysiology For The Health Professions 5th Edition by Vanmeterjosephestradakmbaizgpyj100% (25)
- SplenectomyDocument5 pagesSplenectomysharjil chaudhryNo ratings yet
- Study of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsDocument4 pagesStudy of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsTri UtomoNo ratings yet
- Q&A FractureDocument13 pagesQ&A FractureRed JimenoNo ratings yet
- Staffing July 10 12 2022Document5 pagesStaffing July 10 12 2022Kasandra Dawn Moquia BerisoNo ratings yet
- 1 - RF Report ?Document3 pages1 - RF Report ?مدى القحطانيNo ratings yet
- Pio DermaDocument23 pagesPio Dermabla01No ratings yet
- Dazai OsamuDocument8 pagesDazai OsamuzamatinNo ratings yet
- Graft Versus Host Disease..Document2 pagesGraft Versus Host Disease..Sakawath HosainNo ratings yet
- Jandy Aqualink RS Owners ManualDocument88 pagesJandy Aqualink RS Owners ManualAeres707No ratings yet
- Case Study CHNDocument23 pagesCase Study CHNKramer Dialola LacsonNo ratings yet
- Dyspnea Fear Loathing and PhysiologyDocument20 pagesDyspnea Fear Loathing and PhysiologyMayracpp.16No ratings yet
- 2002 July Plab EmqDocument12 pages2002 July Plab EmqsunjaehNo ratings yet
- Nasm One Repetition Max Conversion (Irm) Chart - (PDF-34k)Document4 pagesNasm One Repetition Max Conversion (Irm) Chart - (PDF-34k)J. FluellynNo ratings yet
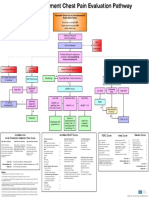
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- ProjectDocument3 pagesProjectAnshul PaunikarNo ratings yet
- Lug Star Trek RPG Netbook - An Open Mind - Mindmelds and Empaths - The Psionics SourcebookDocument118 pagesLug Star Trek RPG Netbook - An Open Mind - Mindmelds and Empaths - The Psionics SourcebookMax Hertzog100% (3)
- Bhagatwala Et Al 2015, Indications and ContraindicationsDocument27 pagesBhagatwala Et Al 2015, Indications and Contraindicationsedo adimastaNo ratings yet