You might also like
- Evaluation of Implant Designs and Materials Used in The MaxiDocument48 pagesEvaluation of Implant Designs and Materials Used in The MaxiNikita AggarwalNo ratings yet
- Implant Designs & Materials For MFPDocument40 pagesImplant Designs & Materials For MFPSpandana100% (1)
- A Simplified Method For The Fabrication of Obturator:a Case ReportDocument4 pagesA Simplified Method For The Fabrication of Obturator:a Case ReportinventionjournalsNo ratings yet
- Maxillofacial-Prosthodontics 002 Jan 2012Document118 pagesMaxillofacial-Prosthodontics 002 Jan 2012Mohsin Habib100% (2)
- Contemporary Implant Dentistry: Chapter 14 of Contemporary Oral and Maxillofacial Surgery By: DrarashkhojastehDocument65 pagesContemporary Implant Dentistry: Chapter 14 of Contemporary Oral and Maxillofacial Surgery By: DrarashkhojastehRawa Omar100% (1)
- Ocular ProsthesisDocument28 pagesOcular ProsthesisrajaniNo ratings yet
- Cataract And Small Pupil Management Manual Techniques: 2022, #1From EverandCataract And Small Pupil Management Manual Techniques: 2022, #1No ratings yet
- Eye For An Eye: Ocular Prosthesis - A Case ReportDocument8 pagesEye For An Eye: Ocular Prosthesis - A Case ReportSkAliHassanNo ratings yet
- Lecture 5Document53 pagesLecture 5Haneen Al-HajjNo ratings yet
- 11 Retention of Maxillofacial Prosthesis Fayad PDFDocument7 pages11 Retention of Maxillofacial Prosthesis Fayad PDFMostafa Fayad50% (2)
- ImplantDocument9 pagesImplantKhaled Abo ZaidNo ratings yet
- Retentive Aids in Maxillofacial ProsthesisDocument109 pagesRetentive Aids in Maxillofacial ProsthesisEnu KambojNo ratings yet
- Cabigas, Mary Rose (Manuscript) CRANIOPLASTYDocument5 pagesCabigas, Mary Rose (Manuscript) CRANIOPLASTYMa. Ydela MeradoresNo ratings yet
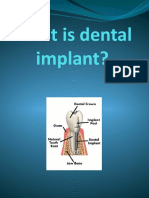
- What Is Dental ImplantDocument14 pagesWhat Is Dental ImplantFaleh ZahrawiNo ratings yet
- Dental Implants PerioDocument81 pagesDental Implants PerioSaba KhanNo ratings yet
- Maxillofacial Prosthesis &materialsDocument7 pagesMaxillofacial Prosthesis &materialsطبطب صالحNo ratings yet
- Retentive Aids in Maxillofacial Prosthes PDFDocument4 pagesRetentive Aids in Maxillofacial Prosthes PDFmaha mohNo ratings yet
- Prosthodontic Management of Compromised Ridges and SituationsDocument8 pagesProsthodontic Management of Compromised Ridges and SituationsTiwi SitompulNo ratings yet
- Cochlear Implant Surgery Treatment & Management - Medical Therapy, Surgical Therapy, Preoperative DetailsDocument9 pagesCochlear Implant Surgery Treatment & Management - Medical Therapy, Surgical Therapy, Preoperative DetailsFityah UfiNo ratings yet
- Surgical ProceduresDocument20 pagesSurgical ProceduresfheisanzNo ratings yet
- Zygoma ImplantDocument63 pagesZygoma ImplantKristina Robles100% (2)
- Chapter 6 Midi Implant ProcedureDocument9 pagesChapter 6 Midi Implant Procedurezeus_1949No ratings yet
- Crown Lengthening of ToothDocument4 pagesCrown Lengthening of Toothisprikitik3No ratings yet
- EnucleationDocument6 pagesEnucleationRameez SarwarNo ratings yet
- Basic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDocument69 pagesBasic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDrFarha NazNo ratings yet
- Ocular Prosthesis BhavanDocument58 pagesOcular Prosthesis BhavanDrkvpratheep Pratheep100% (1)
- Dental Implants PerioDocument54 pagesDental Implants PerioFourthMolar.com0% (1)
- Implant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoDocument6 pagesImplant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoMelina Nataly Robles AcuñaNo ratings yet
- Maxillofacial Prosthodontics PDFDocument81 pagesMaxillofacial Prosthodontics PDFMøĦãmèd Gämãl GømǮã100% (4)
- Impression Techniques in Removable Partial DentureDocument8 pagesImpression Techniques in Removable Partial DentureLama Nahed100% (2)
- Prosthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportDocument4 pagesProsthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportdedeNo ratings yet
- CCD 4 509Document3 pagesCCD 4 509gbaez.88No ratings yet
- Socket Classification ArticleDocument7 pagesSocket Classification ArticleBerkshire District Dental Society100% (1)
- Imp 521Document149 pagesImp 521Mohamed KilaniNo ratings yet
- Ato ZOrthodontics Vol 21 Retentionand RelapseDocument21 pagesAto ZOrthodontics Vol 21 Retentionand RelapseYusuf DiansyahNo ratings yet
- Immediate Implant in Extraction Socket: by Dr. Yasser BarakaDocument11 pagesImmediate Implant in Extraction Socket: by Dr. Yasser BarakaEsmail AhmedNo ratings yet
- A Technique For Fabrication of An Interim Ocular ProsthesisDocument8 pagesA Technique For Fabrication of An Interim Ocular ProsthesisDeepthi Rajesh100% (1)
- Corrective Phase of Periodontal Therapy (Surgical Phase)Document12 pagesCorrective Phase of Periodontal Therapy (Surgical Phase)Hassan MohamedNo ratings yet
- Prosthodontics SHEET - 2014Document12 pagesProsthodontics SHEET - 2014Yomna NimerNo ratings yet
- ManuscriptDocument3 pagesManuscriptAbhishek Kumar GuptaNo ratings yet
- Oral ImplantologyDocument19 pagesOral ImplantologyKariim AhmadNo ratings yet
- Cataract Extraction (Cataract Surgery)Document17 pagesCataract Extraction (Cataract Surgery)John Rey HesitaNo ratings yet
- A Hollow-Bulb Interim Obturator For Maxillary ResectionDocument3 pagesA Hollow-Bulb Interim Obturator For Maxillary Resectionsiddu76No ratings yet
- Immediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportDocument6 pagesImmediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportBagis Emre GulNo ratings yet
- A Prosthodontic Rehabilitation of A Partial Maxillectomy Patient With Hollow Bulb ObturatorDocument4 pagesA Prosthodontic Rehabilitation of A Partial Maxillectomy Patient With Hollow Bulb ObturatorDentist HereNo ratings yet
- The Socket-Shield Technique at Molar Sites: A Proof-Of-Principle Technique Report. C Schwimer Et Al. JPD 2018:5 (12) 56-60Document33 pagesThe Socket-Shield Technique at Molar Sites: A Proof-Of-Principle Technique Report. C Schwimer Et Al. JPD 2018:5 (12) 56-60rajaniNo ratings yet
- An Innovative Technique For Fabricating A CustomMade Ocular Prosthesis in A Pediatric Patient A Case ReportDocument4 pagesAn Innovative Technique For Fabricating A CustomMade Ocular Prosthesis in A Pediatric Patient A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Prosthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesDocument6 pagesProsthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesVero AngelNo ratings yet
- Case Report Band and Loop: A Case Report: Gurkiran Kaur, Garima ChoudharyDocument6 pagesCase Report Band and Loop: A Case Report: Gurkiran Kaur, Garima Choudharyبسمة رياض عبد الستارNo ratings yet
- Oculofacial Plastic and Orbital SurgeryDocument14 pagesOculofacial Plastic and Orbital SurgeryTakwinNo ratings yet
- Maxillary ObturatorDocument79 pagesMaxillary ObturatorAmit KhattakNo ratings yet
- Theme 2 - Partial Acrylic Removable Denture: Maxilla LimitsDocument3 pagesTheme 2 - Partial Acrylic Removable Denture: Maxilla LimitsShany SchwarzwaldNo ratings yet
- Microsoft Word - Vital Pulp TherapyDocument11 pagesMicrosoft Word - Vital Pulp TherapyZeinab Mohamed MorsyNo ratings yet
- Intro +obturators TechDocument26 pagesIntro +obturators Techreem eltyebNo ratings yet
- Single ToothReplacementintheAnteriorMaxillaDocument14 pagesSingle ToothReplacementintheAnteriorMaxillaSteffany BernalNo ratings yet
- 05 EcceDocument9 pages05 EccebebibebihoNo ratings yet
- Rehabilitaton of Nose Using Silicone Based Maxillofacial ProsthesisDocument3 pagesRehabilitaton of Nose Using Silicone Based Maxillofacial ProsthesisOboroc IrinaNo ratings yet
- Clasificación Simpleficada de AlveólosDocument7 pagesClasificación Simpleficada de AlveólosDaniel LazoNo ratings yet
- Basic ImplantologyDocument1 pageBasic ImplantologyjoephinNo ratings yet
- DestinationsDocument1 pageDestinationsjoephinNo ratings yet
- Brochure - NEWDocument7 pagesBrochure - NEWjoephinNo ratings yet
- IDA CDE OfferDocument1 pageIDA CDE OfferjoephinNo ratings yet
- 3D DSDDocument1 page3D DSDjoephinNo ratings yet
- 1st CallDocument1 page1st CalljoephinNo ratings yet
- ALL CERAMIC RESTORATION WordDocument37 pagesALL CERAMIC RESTORATION WordjoephinNo ratings yet
- Pre-Clinical Work : S.No Name of The Student Year of StudyDocument3 pagesPre-Clinical Work : S.No Name of The Student Year of StudyjoephinNo ratings yet
- Basic ImplantologyDocument1 pageBasic ImplantologyjoephinNo ratings yet
- Adin Implants: (Israel)Document3 pagesAdin Implants: (Israel)joephinNo ratings yet
- Department of Prosthodontics and Crown and Bridge: 1 Year MDS ScheduleDocument2 pagesDepartment of Prosthodontics and Crown and Bridge: 1 Year MDS SchedulejoephinNo ratings yet
- Case Report Magnet Retained Detachable Cheek Plumper: Innovation Personified - A Case ReportDocument5 pagesCase Report Magnet Retained Detachable Cheek Plumper: Innovation Personified - A Case ReportjoephinNo ratings yet
- The Tamil Nadu Dr. M.G.R. Medical University, ChennaiDocument7 pagesThe Tamil Nadu Dr. M.G.R. Medical University, ChennaijoephinNo ratings yet
- Dental Casting DefectsDocument86 pagesDental Casting Defectsdennu101100% (3)
- Case Report: Magnet-Retained Facial Prosthesis Combined With Maxillary ObturatorDocument6 pagesCase Report: Magnet-Retained Facial Prosthesis Combined With Maxillary ObturatorjoephinNo ratings yet
- Castingprocedures 181226043739 PDFDocument178 pagesCastingprocedures 181226043739 PDFjoephinNo ratings yet
- Castingprocedures 181226043739 PDFDocument178 pagesCastingprocedures 181226043739 PDFjoephinNo ratings yet
- BCS Multi Unit Course BangaloreDocument7 pagesBCS Multi Unit Course BangalorejoephinNo ratings yet
- JOMIDADocument2 pagesJOMIDAjoephinNo ratings yet
- Noble Implant Impression TechniquesDocument2 pagesNoble Implant Impression TechniquesVero AngelNo ratings yet
- Rehabilitation of A Complete Maxillectomy Patient: A Case Report of Osteomyelitis of MaxillaDocument6 pagesRehabilitation of A Complete Maxillectomy Patient: A Case Report of Osteomyelitis of MaxillajoephinNo ratings yet
- Case Report Magnet Retained Detachable Cheek Plumper: Innovation Personified - A Case ReportDocument5 pagesCase Report Magnet Retained Detachable Cheek Plumper: Innovation Personified - A Case ReportjoephinNo ratings yet
- Jap 2 58Document3 pagesJap 2 58joephinNo ratings yet
- Implant CourseDocument1 pageImplant CoursejoephinNo ratings yet
- Eview: Retentive Aids in Maxillofacial Prosthodontics - A ReviewDocument5 pagesEview: Retentive Aids in Maxillofacial Prosthodontics - A ReviewjoephinNo ratings yet
- Castingprocedure 141012113403 Conversion Gate01Document103 pagesCastingprocedure 141012113403 Conversion Gate01joephinNo ratings yet
- Bite SplintsDocument15 pagesBite SplintsAmit Parmar100% (1)
- Basalimplants 3 130724225029 Phpapp02Document26 pagesBasalimplants 3 130724225029 Phpapp02joephinNo ratings yet
- Treatment of The Grossly Resorbed Mandibular Ridge2Document17 pagesTreatment of The Grossly Resorbed Mandibular Ridge2joephinNo ratings yet
- Taking Calvarial Grafts - Tools and Techniques - VI. The Splitting of A Parietal Bone "Flap"Document15 pagesTaking Calvarial Grafts - Tools and Techniques - VI. The Splitting of A Parietal Bone "Flap"MikeunoeNo ratings yet
- Occular ProsthesisDocument30 pagesOccular ProsthesisPavithra BalasubramaniyamNo ratings yet
- Ocular ProstheticsDocument2 pagesOcular ProstheticsEshiramhe AugustineNo ratings yet
- Quality of Life Assessment of Patients Utilizing Orbital Implant Supported ProsthesesDocument6 pagesQuality of Life Assessment of Patients Utilizing Orbital Implant Supported ProsthesesBagis Emre GulNo ratings yet
- PanophthalmitisDocument31 pagesPanophthalmitisRizty Mayang FachleviNo ratings yet
- Artificial EyeDocument24 pagesArtificial Eyeapoorva1509No ratings yet
- 1ramya Artificial Eye Seminar PPT FinalisedDocument18 pages1ramya Artificial Eye Seminar PPT FinalisedShafiyaanNo ratings yet
- Vis-Con 2024-1Document15 pagesVis-Con 2024-1Deepthi Chandra Shekar SuraNo ratings yet
- 15.ocular ProsthesisDocument156 pages15.ocular ProsthesisrajaniNo ratings yet
- Eye Prosthesis: by G. Vineeth Iii MdsDocument20 pagesEye Prosthesis: by G. Vineeth Iii MdsVinay SahuNo ratings yet
- Pine2015 Book ClinicalOcularProstheticsDocument364 pagesPine2015 Book ClinicalOcularProstheticsCamero Reyes Ariana RubíNo ratings yet
- Eye ProsthesesDocument75 pagesEye ProsthesesNiharika SabharwalNo ratings yet
- MaxillofacialDocument11 pagesMaxillofacialManjeevNo ratings yet
- Eye For An Eye: Ocular Prosthesis - A Case ReportDocument8 pagesEye For An Eye: Ocular Prosthesis - A Case ReportSkAliHassanNo ratings yet
- EnucleationDocument6 pagesEnucleationRameez SarwarNo ratings yet
- Ocular ProsthesisDocument80 pagesOcular ProsthesisPriyaAgrawalNo ratings yet
- Lesson Plan in Physical ScienceDocument12 pagesLesson Plan in Physical ScienceRhisia RaborNo ratings yet
- ENUCLEATIONDocument3 pagesENUCLEATIONTessa BingaroNo ratings yet
- IJPRDDEC2013EYEPROSTHESISDocument6 pagesIJPRDDEC2013EYEPROSTHESISSahana RangarajanNo ratings yet
- History of BiomaterialDocument1 pageHistory of BiomaterialALEJANDRA LOPEZNo ratings yet
- Case Report: Total Lower Eyelid Reconstruction With A Prefabricated Flap Using Auricular CartilageDocument7 pagesCase Report: Total Lower Eyelid Reconstruction With A Prefabricated Flap Using Auricular CartilageFaisal HameedNo ratings yet
- Allegheny General Hospital ArticleDocument28 pagesAllegheny General Hospital Articleem245706No ratings yet
- ENUCLEATIONDocument14 pagesENUCLEATIONBlessy SebastianNo ratings yet
- Anophthalmic Socket: OculoplastyDocument5 pagesAnophthalmic Socket: OculoplastySariShafadenaSiregarNo ratings yet
- KDJVol33No4 KeralaDentalJournal 2Document62 pagesKDJVol33No4 KeralaDentalJournal 2Loly SinagaNo ratings yet
- Ocular ProsthesisDocument3 pagesOcular ProsthesisAmar BhochhibhoyaNo ratings yet
- Eye Cancer (Melanoma and Lymphoma)Document42 pagesEye Cancer (Melanoma and Lymphoma)Vera AvliwaniNo ratings yet
- Ocular Prosthesis BhavanDocument58 pagesOcular Prosthesis BhavanDrkvpratheep Pratheep100% (1)
- Orbital ProsthesisDocument5 pagesOrbital ProsthesisdrsmritiNo ratings yet
- Fish SurgeryDocument22 pagesFish SurgeryCatalina TrujilloNo ratings yet